You’re home. The ride back through Boston felt longer than usual, every pothole mattered, and now the discharge paperwork is sitting on the counter while the important questions start. How much should you move today? What pain is normal? When do you push, and when do you stop?
That’s where post surgical rehab Boston needs to be more than a generic handout. Active people in this city don’t just want to heal. They want to get back to commuting, lifting, running along the Charles, climbing brownstone stairs, carrying groceries through Back Bay, and returning to work without feeling fragile. The safest recoveries usually come from a phased plan that respects healing tissue while building momentum early.
A lot of patients make the same mistake in one of two directions. They either do too little because they’re scared to move, or too much because they’re eager to get back fast. Neither works well. The sweet spot is structured, supervised progression, especially after orthopedic and sports-related surgery.
Your Post-Op Guide The First 72 Hours
The first three days at home often feel disjointed. You’re tired, sore, a little foggy, and every simple task suddenly takes planning. That’s normal. The key is to make these first hours boring, safe, and consistent.

What to do right away
Start with the basics your surgeon already gave you, then tighten up the routine.
- Protect the surgical area: Follow the exact precautions for weight-bearing, brace use, sling use, bending, twisting, or lifting. If your paperwork and your memory don’t match, trust the paperwork and call the surgeon’s office.
- Set a schedule: Take medication as prescribed, ice as instructed, and change position regularly. Recovery goes better when you don’t wait until pain spikes.
- Move in short bouts: Short, approved movement helps circulation and reduces the stiffness that creeps in fast after surgery.
- Keep essentials at waist level: Water, meds, charger, snacks, and pillows should be easy to reach. You shouldn’t be climbing, stretching overhead, or digging through bags today.
If your procedure involved pelvic, colorectal, or nearby tissues, comfort strategies matter just as much as movement. Some patients also benefit from practical guidance on support for cancer treatment anal pain when sitting and hygiene become part of the recovery challenge.
The first movements that usually help
Most patients tolerate a few simple patterns well, assuming they’re cleared by the surgeon.
- Ankle pumps help keep blood moving when you’re spending more time resting.
- Gentle walking indoors breaks up long periods of sitting or lying down.
- Position changes every so often reduce pressure and stiffness.
- Deep breaths can help if you’ve been guarding and staying rigid.
Practical rule: If a movement causes sharp pain, a sudden catch, or a clear loss of control, stop and reassess. Soreness is common. A strong warning signal is different.
What not to do
The first 72 hours are not the time to test your toughness.
| Avoid this | Why it backfires |
|---|---|
| Long stretches in one position | Stiffness and swelling build quickly |
| Unapproved exercises from social media | They may ignore your exact surgical precautions |
| Fast transfers in and out of bed | Rushed twisting and pulling can irritate healing tissue |
| “Catching up” with activity on a good day | Recovery isn’t linear, and overdoing it often shows up the next morning |
Boston homes add their own complications. Narrow stairs, slick entryways, and old flooring aren’t ideal when you’re groggy and guarded. Clear a path. Wear stable shoes or socks with grip. If you live on Beacon Hill or in a walk-up, plan every trip up and down the stairs before you start moving.
Red flags that deserve a call
Call your surgeon if pain suddenly escalates, if the incision looks more irritated than expected, or if something feels distinctly wrong rather than a mild ache. A good recovery requires patience, but it also requires paying attention.
Phase One Recovery Gentle Mobility and Protection
The first month is about controlled motion, not proving anything. Healing tissue needs protection, but the rest of your body still needs a job to do. That job is gentle activation, circulation, and keeping good movement habits from disappearing.

Patients usually feel better once they understand this phase. You are not “behind” because you’re doing small exercises. Early rehab is supposed to look basic. The basics are what prevent the compensations that become harder to undo later.
What phase one should look like
This phase usually includes low-load, surgeon-approved movement that restores confidence without irritating the repair.
- Ankle pumps and walking intervals: These support circulation and keep your day from turning into complete inactivity.
- Quad sets or glute squeezes: These help maintain muscle recruitment when bigger movements aren’t ready yet.
- Gentle range of motion drills: Only if cleared, and only within the limits set for your procedure.
- Position practice: Standing tall, sitting well, and getting in and out of bed safely are part of rehab too.
A study following 68 patients found that 49% had not fully recovered physical functioning three months after surgery, while patients with higher physical activity levels at one month after discharge had better outcomes through three months. Median active time rose from 13 to 46 minutes per day during hospitalization, then to 138 minutes at one month and 159 minutes by three months, which supports the value of early, progressive activity after surgery (post-discharge physical activity and recovery outcomes).
That doesn’t mean you should go chase step counts on day five. It means smart movement early matters.
Boston-specific movement problems
Daily life in Boston creates little traps during this stage.
- Brownstone stairs: Use the rail. Slow down. Carry less than you think you can.
- Desk work in the Seaport or Downtown: Start with short sitting blocks and change position before pain forces you to.
- Public transit: If standing balance is off, don’t test it on a jerky Green Line ride too soon.
- Cobblestones and uneven sidewalks: Short, careful walks beat one ambitious outdoor walk that leaves you flared up.
Recovery gets smoother when your day is built around repeatable wins. Walk well. Sit well. Sleep better. Then add more.
If your surgery involved the shoulder, the rhythm of progression matters just as much as the exercises themselves. Our practical guide to physical therapy after rotator cuff surgery covers that protective early period in more detail.
A quick visual can help if you’re trying to picture what controlled rehab movement looks like at home:
What patients get wrong in phase one
The most common mistake isn’t laziness. It’s impatience.
Some people turn every home exercise session into a workout. Others stop moving because one day felt more sore than the day before. Neither response is useful. What works is consistency, small progressions, and a clear understanding of what pain means for your specific surgery.
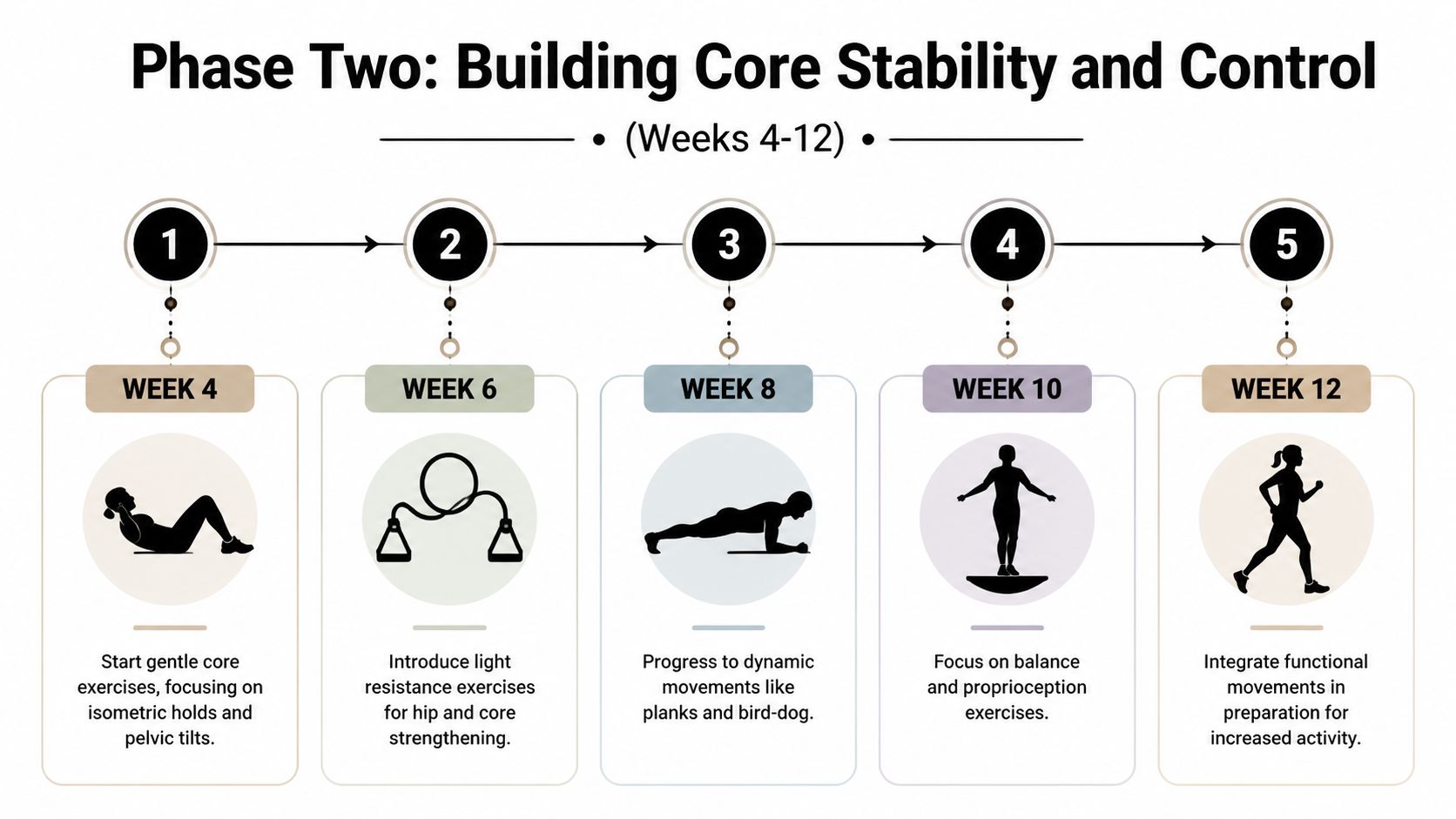
Phase Two Rehab Building Core Stability and Control
At some point, protection alone stops being enough. Once your surgeon clears the next stage, rehab shifts toward control. Here, patients start feeling stronger, but it’s also when sloppy movement can sneak in.
Core stability after surgery doesn’t mean doing sit-ups. It means learning how to organize your trunk, hips, shoulder girdle, or lower body so force goes where it should. Without that, people return to activity with compensations that look small but keep feeding pain.
What changes in this phase
Early healing is quieter. This phase gets more active and more technical.
You may start working on:
- Bracing patterns that teach you to control your trunk without breath-holding
- Bridges for posterior chain support
- Bird-dogs to coordinate trunk and limb control
- Hip strengthening so walking, stairs, and transfers stop dumping stress into one area
- Balance drills that rebuild confidence before higher-level movement returns
Why structure matters here
This phase works best when the progression is deliberate. Enhanced Recovery After Surgery, or ERAS, emphasizes that idea across the surgical timeline. In a meta-analysis of 74 RCTs involving 9,076 patients, ERAS protocols reduced hospital length of stay by 1.88 days and reduced complications by 29%, with early mobilization included in 71% of studies (ERAS meta-analysis findings).
That evidence lines up with what we see clinically. People do better when rehab is organized, paced, and coordinated instead of improvised.
Where one-on-one guidance matters most
This is also the phase where form starts to matter more than effort. A patient can do a bridge while gripping through the low back instead of using the hips. They can do a bird-dog while rotating and hinging around the wrong segments. They can walk farther but still move poorly.
Better movement control usually feels less dramatic than brute-force exercise, but it’s what makes the next phase possible.
For some post-op patients, aquatic therapy is useful here because water reduces load while still letting you work on gait, control, and confidence. Others need hands-on cueing, manual therapy, or a clearer home plan. Some use a clinic like Joint Ventures Physical Therapy for one-on-one outpatient progression after discharge, especially when the goal is a return to sport, commuting, or gym training rather than basic household mobility.
If you’re moving through recovery after a lower-extremity procedure, this article on physical therapy after hip replacement is a good companion for understanding how structured strengthening and mobility progress over time.
What doesn’t work
A rushed jump into “real exercise” usually backfires. So does staying stuck in ultra-gentle rehab for too long.
| Helpful progression | Unhelpful progression |
|---|---|
| Controlled loading with clear technique | Random strength work based on what feels hard |
| Criteria-based increases | Calendar-based jumps because “it’s been a few weeks” |
| Feedback on compensations | Assuming more reps automatically means more progress |
Phase Three Returning to Your Boston Life
After the early milestones, most patients ask a better question. Not “When am I healed?” but “How do I get back to my actual life without blowing this up?”
That’s the right question. This phase is less about the procedure and more about the demands waiting for you outside the clinic.

The runner on the Esplanade
The Boston runner often feels good enough before they’re ready enough. They can walk, maybe jog a little, and the temptation is to test a loop along the Charles. The issue isn’t motivation. The issue is load tolerance.
A safe return usually starts with criteria. Can you tolerate impact drills? Can you control single-leg loading? Does your gait stay clean as fatigue builds? That’s where a running evaluation matters more than a guess.
The desk worker in the Seaport
Another patient profile is the professional who returns to a chair, a laptop, and long blocks of stillness before their body is ready. They don’t need a return-to-sport protocol first. They need a return-to-work strategy.
That often means:
- Breaking up sitting time before symptoms spike
- Resetting workstation setup so the neck, shoulder, and back aren’t carrying unnecessary strain
- Rebuilding tolerance for commuting including stairs, carrying a bag, and walking on uneven sidewalks
- Adding strength for daily loads so groceries, laundry, and travel don’t become rehab setbacks
The athlete who wants the gym back
For lifters, golfers, and recreational athletes, this stage is about earning complexity. The shoulder patient may need pressing mechanics rebuilt. The knee patient may need landing control before they touch box jumps. The golfer may need rotational strength and sequencing before a full swing feels smart.
Research on phased post-surgical exercise found that a structured program helped patients regain 95% of pre-operative shoulder strength at one and six months, with an 80% return-to-sport rate, compared with 55% in control groups (structured post-surgical exercise findings).
That kind of result comes from progression, not optimism.
A timeline is useful. A readiness test is better.
How readiness actually gets tested
A return to Boston life should be based on what you can demonstrate, not what you hope will be fine.
- Strength has to show up under load.
- Balance and control have to hold up when you’re tired.
- Your movement pattern has to stay clean outside the clinic.
- Your specific goal matters. Running, golf, lifting, and long desk days all stress the body differently.
That’s why post surgical rehab Boston should feel personal. The right final phase for a Fenway-area student athlete doesn’t look like the right final phase for a Financial District commuter or an active parent carrying a toddler up apartment stairs.
Why 1-on-1 Physical Therapy Is Your Key to Success
A home program matters. It just isn’t enough by itself for many post-op patients.
The hard part of surgical recovery usually isn’t knowing that you need to do exercises. It’s knowing whether you’re doing the right exercises, at the right time, with the right technique, and the right amount of load. That’s the gap one-on-one care fills.
Boston has strong hospital rehab and a real outpatient gap
Boston has outstanding inpatient care. Spaulding Rehabilitation Hospital discharges 94.4% of adult inpatient patients back to living in the community within 90 days, which speaks to the value of coordinated rehab systems (Spaulding rehabilitation outcomes). But that still leaves a separate outpatient need for active people who want to return to sport, work, lifting, or higher-level movement.
The outpatient gap matters because post-surgical athletes face a 20-30% higher re-injury rate without sport-specific protocols (Boston-area outpatient rehab gap and re-injury risk). Generic rehab can get someone walking. It may not get them confidently back to cutting, sprinting, swinging, or training.
What a therapist catches that patients often miss
Patients usually notice pain. A skilled therapist also notices the quieter problems:
- Guarding patterns that shift load away from the surgical area and into somewhere else
- Asymmetry during stairs, sit-to-stand, reaching, or single-leg tasks
- Mobility loss that starts small but changes mechanics
- Fear-driven movement where the body moves stiffly even after tissue healing is progressing
Those details matter because compensations become habits fast.
If pain is radiating, numbness is showing up, weakness is increasing, or your function is moving backward instead of forward, get assessed. Waiting often makes the fix more complicated.
Why active patients need more than generic progression
A post-op runner may need gait analysis. A golfer may need rotational assessment or a Titleist evaluation. Someone with dizziness after surgery may need vestibular input before they can return to full activity. A patient with jaw tension, pelvic floor symptoms, or stubborn muscle guarding may need care that a standard protocol doesn’t address.
That’s why broad orthopedic guidance alone often falls short. If you want a wider view of this category, our page on orthopedic physical therapy is a useful starting point.
Going it alone usually creates one of two outcomes
| Approach | Typical result |
|---|---|
| Too cautious for too long | Ongoing weakness, stiffness, and loss of confidence |
| Too aggressive too early | Pain flare, swelling, compensation, or setback |
| Supervised, criteria-based progression | Safer return to real activity |
One-on-one care isn’t about making rehab feel fancy. It’s about making rehab accurate.
Take the Next Step in Your Recovery in Boston
Surgery changes the timeline, but it doesn’t change the goal. You still want your life back. The route there is a phased plan that respects healing, restores movement, rebuilds strength, and tests readiness before you jump back into the things that matter.
That’s especially true in Boston. This city asks a lot from your body. You walk more, climb more stairs, carry more through tighter spaces, and often try to return quickly because work, family, and training schedules don’t slow down much. Good rehab meets that reality instead of pretending recovery happens in a vacuum.
What to do next
If you’re early after surgery, book an evaluation before bad habits settle in. If you’re stuck in the middle, get help identifying what’s limiting progress. If you’re months out but still don’t trust the joint, limb, or movement, that’s also a reason to be seen.
Useful next steps often include:
- Clarifying your precautions and timeline
- Building a realistic home program
- Testing movement quality, not just pain levels
- Planning for your real-world goal, whether that’s returning to the gym, commuting comfortably, running, or playing golf
Some patients also like having a broader healing checklist outside PT. For general recovery habits after a procedure, Cape Cod Plastic Surgery offers practical guidance on supporting the healing process day to day.
Where local care helps most
Boston-area outpatient rehab works best when the clinician understands the life you’re returning to. Back Bay walking demands aren’t the same as a car-based suburb. A Kenmore student athlete doesn’t need the same progression as a Seaport professional recovering for long desk days and travel. A strong plan should reflect that.
For deeper educational content on injury anatomy, surgery recovery concepts, and condition-specific background, visit Highbar Health at highbarhealth.com. That’s the right place for broader clinical education, while your local plan should stay focused on your Boston-specific recovery and return to activity.
If you’re ready to move forward, schedule a one-on-one evaluation in Back Bay, Kenmore Square, Fort Point/Seaport, or Downtown Boston and start building a recovery plan that fits the way you live.
If you're looking for Joint Ventures Physical Therapy, book a one-on-one post-surgical evaluation at a Greater Boston location and get a plan built around your surgery, your neighborhood, and your return-to-life goals.


