A lot of Boston shoulder pain doesn't start with a dramatic injury. It starts with a laptop in the Seaport, a long Red Line commute, a phone held between ear and shoulder, or mile after mile of marathon training with a stiff upper back and tired postural muscles. Then one day you reach overhead for a backpack, finish a swim, or settle into bed and notice that nagging ache behind the shoulder blade.
That's the type of problem prone horizontal abduction often helps address. In clinic, this isn't just a random “upper back exercise.” It's a targeted movement we use to build control in the back of the shoulder and around the shoulder blade, especially when someone has poor posture tolerance, shoulder fatigue, or recurring irritation with reaching, lifting, or sport.
For a lot of active adults in Boston, the appeal is simple. The exercise looks modest, but when it's coached well, it trains the exact kind of low-load stability that supports desk work, running posture, lifting, racket sports, and return to overhead activity. If you're already dealing with an irritated shoulder, our shoulder pain physical therapy in Back Bay guide can help you decide when exercise alone is enough and when an evaluation makes more sense.
Your Guide to Fixing Shoulder Pain in Boston
A Back Bay consultant closes the laptop after ten hours of meetings and feels a dull pull along the back of the shoulder. A runner training along the Charles notices the arm swing getting tight by mile eight. A college athlete comes back to lifting and finds that pressing feels fine for a few reps, then the shoulder starts to pinch.
In the clinic, those stories often trace back to the same issue. The shoulder can move, but it does not hold position well under load or fatigue. The upper trap and neck step in early. The muscles on the back side of the shoulder and shoulder blade lag behind, so everyday work, sport, and training start to feel more irritating than they should.
Prone horizontal abduction shows up often in rehab because it gives us a clean way to train that missing control. The goal is not heavy strength. The goal is better timing, better endurance, and less compensation through the neck and upper shoulders. That matters for Boston patients who spend the week at a desk, then ask the same body to handle rowing, tennis, lifting, or marathon prep on the weekend.
I use this exercise a lot for desk workers with postural fatigue, runners who carry tension through the upper quarter, and athletes who need shoulder stability without aggravating symptoms. It also fits well into broader care when shoulder pain overlaps with neck tension, jaw clenching, or training errors. That crossover is common in our Boston population, which is one reason shoulder rehab at Joint Ventures often sits alongside sports performance work and, in the right case, TMJ-focused treatment.
The catch is that this exercise is easy to do poorly. Online demos often make it look like a simple "T" raise. In practice, the details decide whether you train the right tissues or just feed the shrugging pattern that already irritates the shoulder.
If you feel this mostly in the neck, stop and reset.
For patients trying to decide whether home exercise is enough or whether the shoulder needs a closer look, our shoulder pain physical therapy guide for Back Bay patients lays out the signs I would take seriously.
Why This Key Move Unlocks Shoulder Stability
A shoulder that feels strong during a lift or stable at mile 18 usually has one thing in common. The shoulder blade gives the arm a dependable base instead of drifting into a shrug, a forward tip, or a neck-driven compensation pattern.
Prone horizontal abduction helps build that base. It targets the posterior shoulder and scapular muscles that often lose endurance in Boston patients who split their week between laptop work, the T, and higher training loads on weekends. That combination shows up all the time in clinic. The office worker with ache at the top of the shoulder often has the same control problem as the runner whose arm swing tightens late in a long run.
When this exercise is done well, the goal is not just to raise the arm. The goal is to improve how the lower trap, middle trap, posterior cuff, and scapular stabilizers share the job so the neck does less unnecessary work. That matters for shoulder pain, but it also matters for performance. Runners need efficient arm carriage. Lifters need a better platform overhead. Patients with jaw tension or cervicogenic tightness often do better when the upper quarter stops asking the neck to do everything.

Small form changes change what you train
This is one reason I rarely hand this out without a few specific cues. A slight change in trunk position, shoulder rotation, or arm path can shift the effort away from the tissues we want and back into the upper trap.
A JKEMA study on prone shoulder horizontal abduction found that setup changes influenced which scapular muscles were emphasized, including greater lower trapezius activity in one prone variation and lower upper trapezius activity in a sitting variation. Clinically, that matters. If someone already lives in a shrugged posture, I may choose the version that keeps the neck quieter before progressing to a more demanding prone setup.
That trade-off is the real point. There is no single perfect variation for every shoulder. There is a right variation for the problem in front of you.
Why that matters for Boston patients
In Boston, shoulder issues are rarely isolated from the rest of life.
- For desk workers: this exercise can help restore posterior shoulder endurance that fades after hours of keyboard and mouse use.
- For runners and triathletes: it can improve arm swing control and reduce the upper-quarter tension that builds during higher-mileage weeks.
- For overhead athletes and lifters: it supports cleaner scapular mechanics without jumping straight to heavy loading.
- For TMJ and neck pain patients: better scapular control can reduce how often the neck and jaw try to stabilize the upper body.
If you want a broader home program around the same goal, our guide to the best exercises for shoulder pain gives more context on where this movement fits.
The shoulder usually feels better when the scapula does its share and the neck stops filling in for it.
How to Perform Prone Horizontal Abduction at Home
This exercise should look controlled and a little boring. That's a good sign. If it turns into a swing, a shrug, or a low back extension drill, you've lost the point.
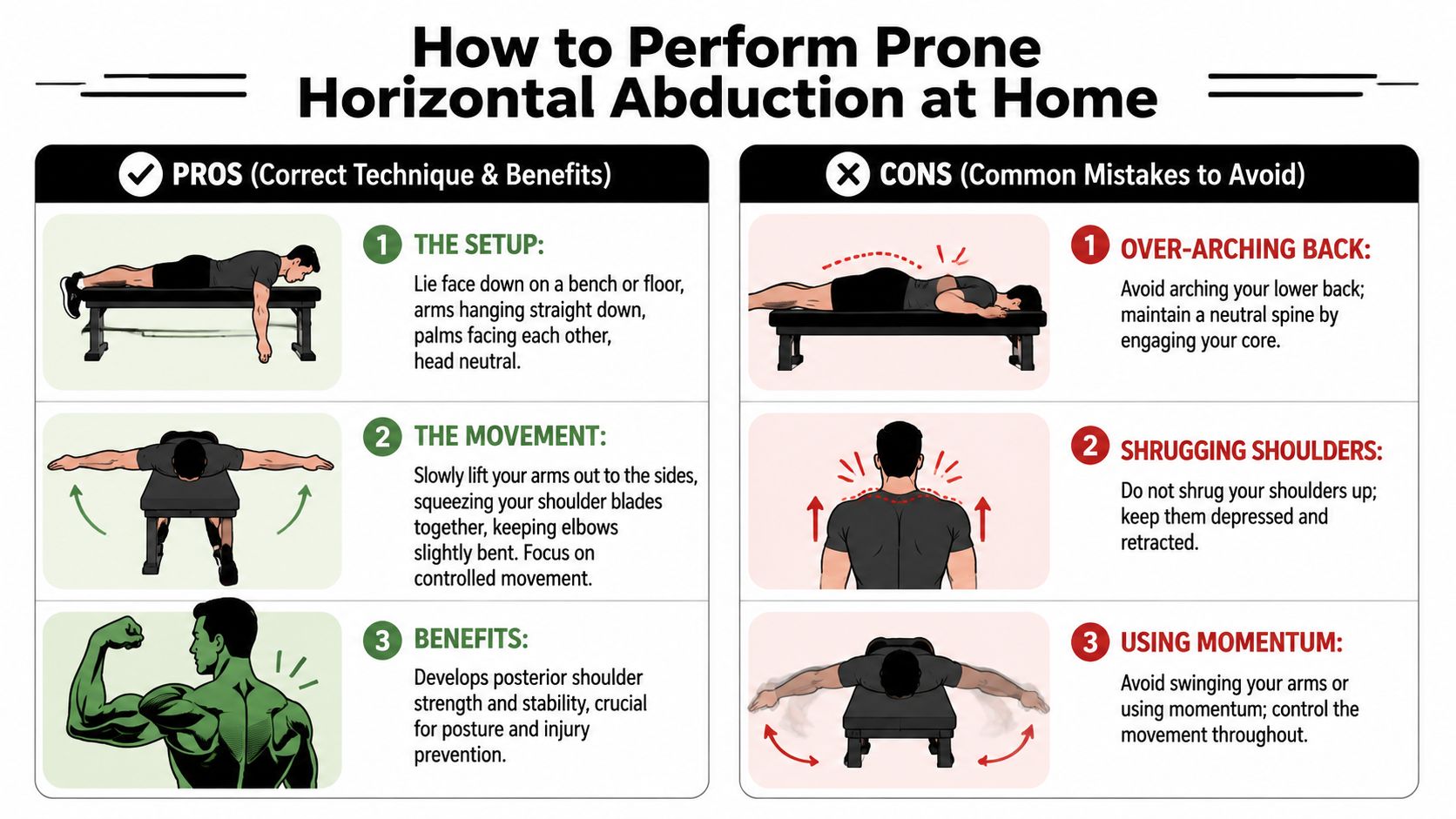
The setup
Lie face down on a bench, bed, or firm surface where your arm can move freely. Keep your chest supported and your neck neutral. Think long through the back of the head rather than lifting your chin to look forward.
Let the working arm hang down first. A thumbs-up position is commonly used because it often helps the shoulder feel cleaner. Start with very light weight, typically about 2.5 to 5 lb, or no weight at all. Expert coaching guidance also notes that progression is usually modest, often staying around 7.5 lb or less, with the arm lifted only to the neutral T position, as shown in this prone horizontal abduction coaching video.
The movement
Before the arm lifts, gently set the shoulder blade with a small scapular retraction. Small is the key word. You're not yanking the shoulder blade back as hard as possible.
Then raise the arm out to the side until it reaches a T position, parallel to the floor. Stop there. Don't keep pulling the arm past the body into shoulder extension.
The best reps usually feel like this:
- Smooth start: The shoulder blade and back of the shoulder begin the motion.
- Quiet neck: Your jaw stays relaxed and your upper traps don't bunch up.
- No momentum: The arm doesn't swing up and drop down.
- Clean stopping point: You reach the T and return with control.
If you want a broader home program, our guide to the best exercises for shoulder pain can help you fit this movement into a larger plan.
Here's a visual demo to pair with the written cues.
Breathing and tempo
Use an easy exhale as the arm lifts. Inhale on the way down. If you hold your breath, you'll often stiffen the neck and rib cage, which makes the movement less precise.
A controlled tempo works better than chasing fatigue. Let the lowering phase be deliberate. That's where a lot of people either drop the arm or lose shoulder position.
Practical rule: If you can't pause briefly at the top without shrugging, the load is too heavy or the range is too high.
What you should feel
You should usually feel work in the back of the shoulder and between the shoulder blade and spine. Mild muscle effort is fine. Sharp pain in the front of the shoulder, pinching, or symptom spread into the neck is not the goal.
If that's what happens, don't keep grinding through reps. That's when a form correction, a different variation, or a different exercise altogether may be the better call.
Common Mistakes and Expert Cues from Our PTs
The biggest mistake with prone horizontal abduction is treating it like a generic “rear delt raise.” In rehab, the question isn't whether you can lift the arm. It's how you lift it, what your body substitutes with, and whether the movement improves the pattern you came in to fix.
When the neck takes over
This is the compensation we see most. The shoulders creep toward the ears, the jaw tightens, and the patient finishes the set feeling more tension near the base of the neck than in the upper back.
Try this cue instead:
- Keep the collarbones wide
- Let the shoulder stay away from the ear
- Make the lift smaller before you make it higher
That usually cleans up the movement faster than telling someone to “squeeze harder.”
When the low back does the lifting
Another common error is turning the rep into a spinal extension strategy. The chest peels up, the ribs flare, and the shoulder never really learns to move on a stable trunk.
A better correction is to think of the trunk as quiet and heavy. The arm moves. The back doesn't perform the rep for you.
Here's a simple contrast.
| Wrong feel | Better feel |
|---|---|
| “I'm arching to get the weight up” | “My chest stays quiet while my arm floats to a T” |
| “I feel it in my neck” | “I feel the back of my shoulder and mid-back” |
| “I'm chasing height” | “I'm stopping where I still have control” |
The scapula shouldn't be frozen
A lot of people hear “stability” and assume the shoulder blade should stay locked down and pinned back. That can help a beginner who has no positional awareness at all, but it becomes limiting if it turns into rigid bracing.
Coaching education points out an important nuance. Beginners usually need to focus on stability first, but a more advanced approach allows controlled scapular motion rather than trying to keep the scapula completely still, as discussed in this clinical coaching video on scapular movement during prone horizontal abduction.
That distinction matters for real life. You don't run, swim, throw, lift, or carry groceries with a frozen shoulder blade. You do those things with coordinated movement.
Early on, think stable. Later, think coordinated.
The cue that often works fastest
If someone keeps muscling through the arm, I'll often change the task completely. Instead of “lift your hand,” I'll coach “slide the shoulder blade slightly, then let the arm follow.” That shifts attention from output to sequence, which is usually what the person was missing in the first place.
How to Progress and Program The Exercise
A common Boston pattern looks like this. Someone spends all week at a laptop in the Seaport, gets neck and shoulder fatigue by Thursday, then tries to jump back into weekend lifting, tennis, or long marathon training runs. The shoulder usually does not need a harder version of prone horizontal abduction first. It needs a version that improves control and can be repeated without flaring symptoms.
The dose depends on the job you need the exercise to do. A runner who wants cleaner arm swing and less upper trap fatigue needs a different plan from a college athlete returning to overhead sport. A patient with jaw and neck tension may also need more attention to posture, breathing, and cervical mechanics, which is something we see often in our TMJ and upper quarter cases at Joint Ventures.
The exercise also fools people. It looks simple, so they load it too early. In practice, this drill works best as low-load training for posterior shoulder endurance, scapular timing, and movement quality.
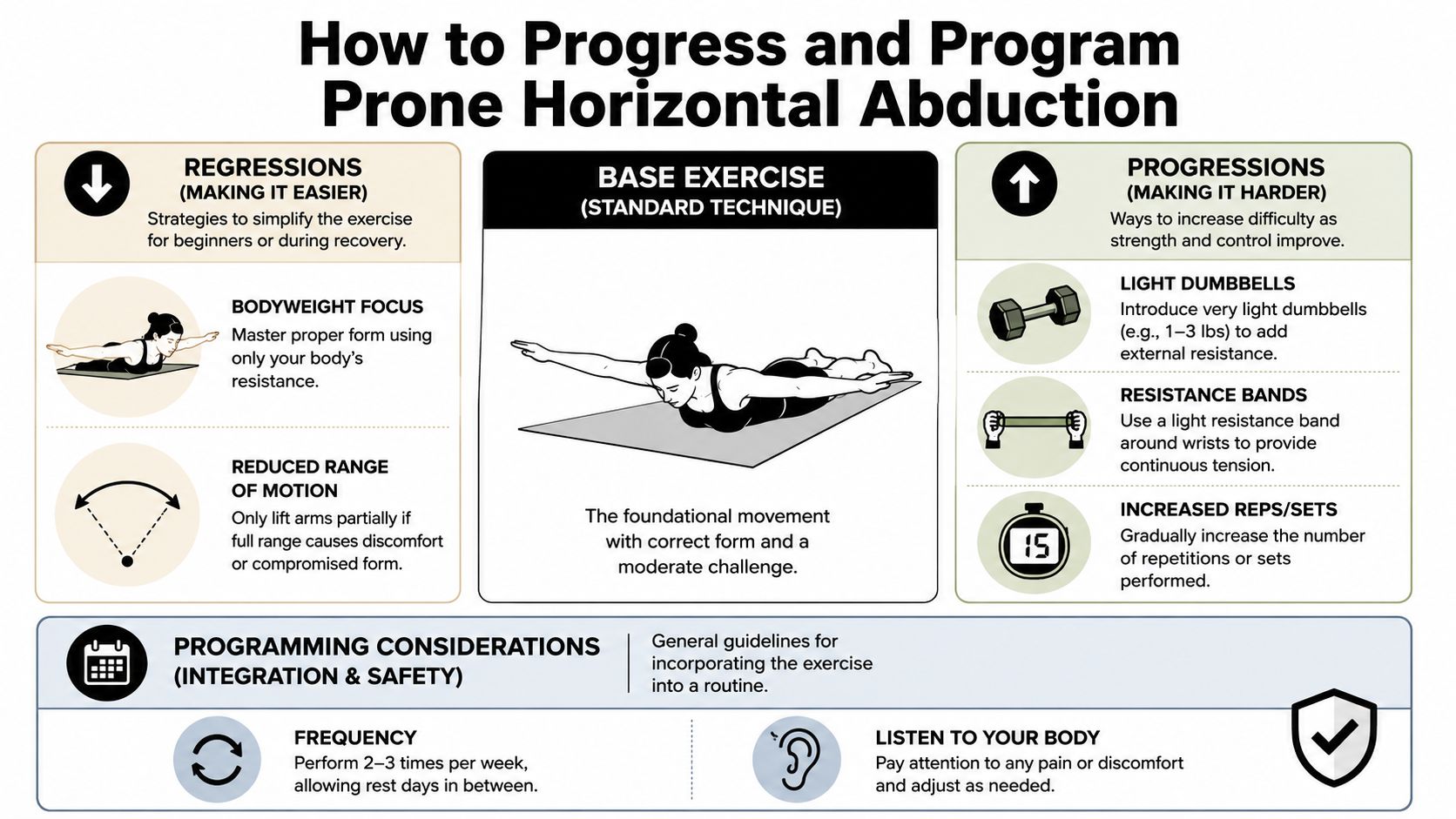
Start with the version you can repeat cleanly
Pick the easiest setup that lets you feel the back of the shoulder and mid-back without neck gripping, trunk rotation, or a big arch through the chest.
- Bodyweight only: Skip the dumbbell until the pattern is consistent.
- Reduced range: Stop at the point where you still have control.
- Supported bent-over variation: This is often a better entry point for desk workers who do not tolerate the prone position well.
- Short sets: End the set when the quality drops.
A practical starting point is 2 to 3 sets of 8 to 15 controlled reps with a very light load or no load at all. If you want more challenge, add a brief pause at the top before you add weight. That usually builds the right kind of effort faster than chasing heavier dumbbells.
If you're pairing this with cuff work, our article on how to strengthen rotator cuff muscles is a good next read.
How to progress it without losing the point
Progression should match the goal.
For a Back Bay desk worker with chronic upper quarter tension, the best next step is often more tolerance: cleaner reps, a longer hold, or one more set without neck compensation. For a runner or swimmer, progression may mean better control into fatigue so the shoulder stays organized late in a session. For an athlete at BU, BC, or one of the local club programs, it may make sense to progress toward positions and speeds that resemble sport.
Use this sequence:
- Build repeatable form. The shoulder should move without the neck taking over.
- Increase time under tension. Add a 2 to 3 second hold or slow the lowering phase.
- Change position or angle. Try a thumbs-up variation, slight incline change, or a supported standing version if it fits the goal better.
- Add light resistance last. More load only helps if the movement still looks controlled.
I rarely rush this progression. A patient can “pass” the exercise with a heavier weight and still miss the reason we prescribed it. Good programming keeps the exercise tied to the core objective, whether that is getting through a workday with less pain, returning to serving in tennis, or holding form deeper into a long run.
One option for Boston patients who want supervision
If you are not sure whether you need a regression, a different arm angle, or a different exercise entirely, Joint Ventures Physical Therapy offers one-on-one orthopedic and upper extremity care across Greater Boston. That matters when the shoulder issue is only part of the picture, which is common in runners, overhead athletes, and patients whose shoulder symptoms overlap with neck or TMJ-related tension.
The best version is the one you can perform well often enough for your shoulder to actually change.
Is This Exercise Right for You in Boston
A common Boston scenario looks like this. You spend the week at a laptop in Back Bay, squeeze in a Charles River run after work, and notice your shoulder and neck tighten up more each month. Or you are a college athlete trying to get back to overhead training without that familiar pinch in the front of the shoulder. Prone horizontal abduction can help in both cases, but only when the exercise matches the reason your shoulder is irritated.
This movement tends to fit people who need better control through the back of the shoulder and shoulder blade. That includes desk workers with postural fatigue, runners whose arm swing comes with extra neck tension, overhead athletes at local schools, and patients building back shoulder function after injury or surgery. In the clinic, I also use it when someone has lost the ability to move the arm well without the upper traps dominating the effort.
It also gives useful information. In a study of competitive swimmers, shoulder horizontal abduction range of motion of 39° or less was associated with a 3.6-fold higher risk of shoulder pain, according to this swimmer shoulder pain study in PMC. For the right patient, that makes the movement more than a strengthening drill. It helps us see whether the shoulder can access the position at all, and whether it does so with control.
When to be cautious
Take a closer look before using this exercise if:
- You feel sharp pain in the position
- Your motion is clearly restricted on one side
- Your shoulder shifts forward or feels unstable
- The movement increases symptoms instead of creating muscular effort
Those details matter in Boston because shoulder pain rarely exists in isolation. A finance professional in the Seaport may need shoulder work plus desk setup changes. A marathon runner may need thoracic mobility and better rib cage control to clean up arm swing. A patient with jaw pain or clenching may need the shoulder and neck addressed alongside TMJ treatment, especially when tension patterns overlap.
If the exercise consistently hurts, feels blocked, or makes the front of the shoulder more irritable, stop forcing it. Get it assessed. Sometimes the right answer is a different arm angle, less range, or a different exercise entirely.
If shoulder pain is limiting your training, workday, sleep, or return to sport, book an evaluation with Joint Ventures Physical Therapy. Our Boston-area clinicians provide one-on-one care for orthopedic injuries, sports rehab, TMJ, workplace ergonomics, and upper extremity issues, with locations convenient to Back Bay, Kenmore Square, Downtown Boston, Fort Point, and surrounding neighborhoods.


