You hear the pop on a soccer field in Cambridge, during a pickup basketball game after work, or halfway through a marathon build on the Charles River. By that night, the knee is swollen, stairs are awkward, and the questions start fast. Do you need surgery, or can you manage this with rehab? If surgery is part of the plan, how long until cutting, sprinting, and full practice are realistic again?
Those are the right questions.
ACL recovery physical therapy Boston patients need is phase-based, measured, and built around real life in this city. A good plan accounts for the knee in front of us, but also for Red Line commutes, walk-up apartments, university schedules, office hours, and the fact that many Boston patients want more than pain relief. They want to get back to competition, long runs, rec leagues, skiing trips, and training without second-guessing every pivot.
Boston gives you access to strong orthopedic and sports medicine care, but access alone does not carry you through recovery. Progress comes from timing the right interventions, hitting objective strength and control markers, and adjusting the program to your goals. At Joint Ventures Physical Therapy, that usually means different conversations for a college athlete in-season, a marathoner trying to protect future training cycles, and an active professional who needs to handle rehab around work and family demands.
For football and soccer athletes who want a practical look at common knee injury patterns and what to watch after contact or twisting injuries, football injury advice from SoccerWares is a useful companion read.
The good news is that ACL rehab is not guesswork. There is a clear path. The hard part is respecting the timeline, meeting the milestones, and avoiding the common Boston mistake of trying to rush from feeling better to being ready. Those are not the same thing.
Navigating Your ACL Injury in Boston
A torn ACL tends to split life into before and after. Before the injury, your week had a rhythm. Running on the Esplanade before work. Lifting in Fenway or the Seaport. Team practices at a local university. Weekend games that were supposed to be routine.
After the injury, your focus gets narrower. Swelling. Stairs. Sleep. How to get across Boston without feeling unstable. For football and soccer athletes who want a practical look at common knee injury patterns and what to watch after contact or twisting injuries, football injury advice from SoccerWares is a useful companion read.
The first good sign is this. ACL rehab has a roadmap. It isn't fast, and it shouldn't be improvised, but it is predictable when the knee is managed in phases and each phase has a clear job.
What Boston patients usually need right away
Some people need surgery soon. Others spend time in prehab first. Some are trying to finish a semester, get through a work deadline, or figure out whether they can manage recovery from an apartment with stairs and no elevator.
That context matters because adherence matters. A strong plan on paper still fails if you can't get to visits, can't manage swelling, or don't understand what you should and should not be doing in the first few weeks.
The athletes who do well usually stop asking, "How fast can I get back?" and start asking, "What does my knee need next?"
What recovery should feel like
Not easy. Not linear. But clear.
You should know what the next milestone is, how it's measured, and why it matters. In Boston, where many patients are balancing sport with work, school, and commuting, that clarity keeps rehab from turning into guesswork.
The First Steps Prehab and Early Post-op Care
Monday morning in Boston, the knee is swollen, the brace keeps slipping, and the walk from the Green Line feels twice as long as it should. That is usually when recovery stops feeling abstract. The first phase has a narrow job. Calm the knee down, restore motion, wake the quad back up, and avoid the early mistakes that slow everything after.

Why prehab matters
A knee that goes into surgery hot, stiff, and swollen usually comes out needing more cleanup. In clinic, the pattern is obvious. Patients who regain full extension early, get swelling under control, and can contract the quad before surgery tend to have a smoother start after surgery.
That does not mean prehab needs to be fancy. It needs to be focused.
The priorities are straightforward:
- Get extension back: Full knee straightening affects walking, standing, and how the quad fires.
- Reduce joint swelling: A swollen knee often shuts the quadriceps down.
- Restore basic muscle activity: Quad sets, straight leg raises when appropriate, and controlled weight shifting help the leg work again.
- Clean up gait: Early limping can become a habit if nobody corrects it.
For active Bostonians, there is a practical trade-off here. Some patients want surgery scheduled as fast as possible. Sometimes that is reasonable. Sometimes a short prehab window saves time overall because the knee is in a better place on day one after surgery.
What to do in the first days after surgery
Early post-op rehab starts quickly. The Boston Sports Medicine ACL rehab protocol notes that formal physical therapy can begin within days after reconstruction. That timeline matters because the first week is where swelling, pain, range of motion, and walking mechanics can either improve steadily or drift in the wrong direction.
In Boston, logistics are part of treatment. A college athlete near Kenmore, a Seaport professional trying to fit visits around work, and a runner managing stairs in a South End walk-up all need the same clinical goals, but the plan has to fit real life or adherence drops. At Joint Ventures Physical Therapy, clinic location and scheduling often matter as much as exercise selection in this phase, especially if you are using crutches and every trip across the city costs energy.
Choose the clinic you can reach consistently. Early rehab rewards repetition.
What early visits should include
The work is simple on paper and exact in practice.
- Swelling management with elevation, compression, light movement, and activity limits that match the knee's response.
- Range of motion work including heel slides and extension-focused positioning.
- Quad reactivation with precise setup, because a compensated rep does not count for much.
- Walking retraining so the hip, ankle, and uninvolved leg do not spend weeks covering for the knee.
- Frequent reassessment because progress can fade fast after a pain spike, a poor night's sleep, or too much time on your feet.
If you want a local breakdown of what that schedule and progression look like, this guide to post-surgical rehab in Boston is a useful reference.
Home exercise consistency matters too, but more is not always better. Early ACL rehab responds well to steady, repeatable work. If you like tracking sessions and gradual increases in workload, Strive Workout Log's guide explains progressive overload well. In the first couple of weeks after ACL surgery, that principle has to be applied carefully. The knee should improve because the dosage is right, not because you forced extra volume.
Common mistakes in this phase
Patients lose time when they wait for swelling to settle on its own, skip crutch or brace adjustments, or push exercises hard enough to irritate the joint every day. I also see avoidable setbacks when patients assume the incision is the main issue. In early ACL rehab, motion loss and quad inhibition are often the bigger problems.
One-on-one attention helps here because the details are small and important. Crutch height changes posture. Brace fit changes confidence. A straight leg raise with lag means the quad is still not doing its job. A knee that is almost straight often is not straight enough.
Early rehab is not dramatic. It is disciplined. Get this phase right, and the rest of the plan has something solid to build on.
Building Your Foundation with Strength and Control
A common Boston rehab moment happens around week six to twelve. The knee looks better, stairs feel easier, and workdays in Back Bay or Cambridge are less awkward. Patients start to wonder if they are ahead of schedule. In clinic, this is often when I have to slow people down and get very specific. Symptom relief is progress, but strength, control, and load tolerance still need to be built.
This phase is where the foundation gets tested. The graft may be healing, but the knee still depends on the quadriceps, hips, trunk, and single-leg control to handle daily demands without compensation. If those systems stay undertrained, the athlete who wants to get back to the Charles, a BU soccer field, or weekend basketball in South Boston usually runs into the same problem. They feel capable before they are physically ready.
Why the quad gets so much attention
Quadriceps weakness is one of the biggest reasons ACL rehab stalls in the middle phase. A patient can have decent range of motion, low pain, and a normal-looking walk, yet still struggle to produce force on the surgical side. That gap shows up later in step-downs, squats, running mechanics, hop testing, and deceleration.
At Joint Ventures, this is why we keep coming back to measurable strength and movement quality instead of guessing based on time since surgery. Calendar milestones help with planning. They should not decide progression on their own.
What this stage usually looks like
The work becomes more demanding, but it should still look controlled. Good ACL rehab in this phase usually includes:
- Closed-chain strengthening: squats, step-ups, split squats, sled work, and leg press progressions based on tolerance
- Single-leg stability work: reach patterns, supported hinging, controlled step-downs, and balance drills that expose side-to-side differences
- Hip and trunk strengthening: frontal-plane control matters because knee valgus and pelvic drift often show up under fatigue
- Conditioning: bike, rower, or other low-impact options to build work capacity without asking for more impact than the knee can handle
- Progressive loading: increasing resistance, depth, complexity, or volume only when the knee stays quiet afterward
For patients who want a local reference for exercise progressions, this article on knee injury recovery exercises gives useful examples.
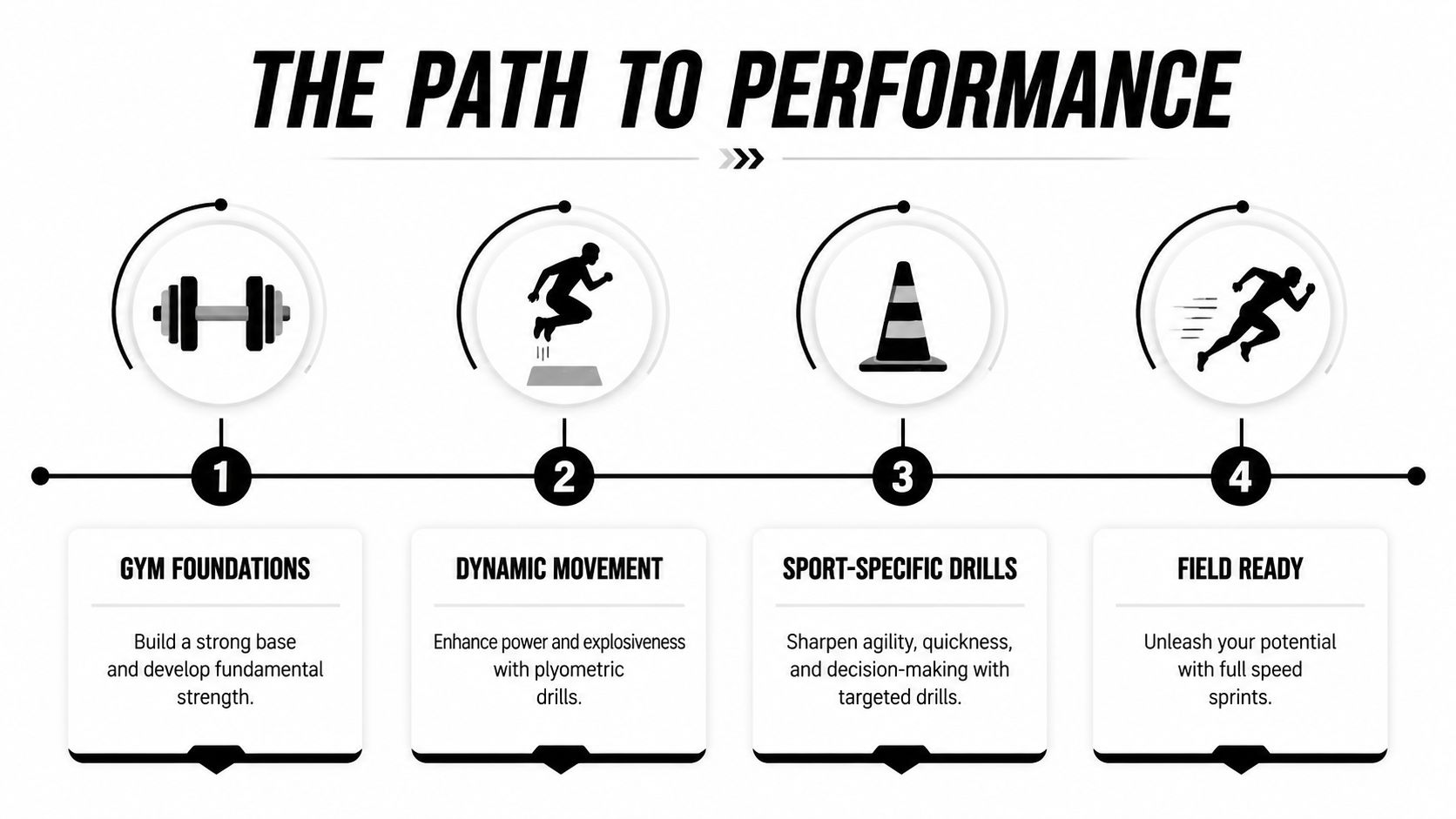
Phases of ACL Rehabilitation at Joint Ventures
| Phase | Typical Timeline | Primary Goals | Key Criteria to Advance |
|---|---|---|---|
| Early protection and motion | Early post-op period | Control swelling, restore extension, improve basic quad activation, normalize walking | Knee is calming down, motion is improving, quad activation is present, gait is becoming cleaner |
| Foundational strength and control | Early to mid rehab | Build quad and hip strength, improve single-leg control, increase exercise tolerance | Strength is progressing, swelling remains controlled, movement quality is consistent |
| Dynamic loading and running prep | Mid to late rehab | Introduce impact preparation, higher-speed force absorption, and sport movement patterns | Strength and control support safe progression into dynamic work |
| Return-to-sport testing and performance | Late rehab | Confirm readiness through functional testing and sport-specific progression | Athlete passes testing battery and demonstrates confidence with sport demands |
Where aquatic therapy can help
Aquatic therapy can be a useful option for Boston patients who are not tolerating land loading well yet. That includes athletes with persistent joint irritation, active adults who need conditioning without repeated impact, and patients who are mentally hesitant to load the surgical leg on land.
The pool does not replace strength training. It gives some patients a better entry point for gait work, supported squatting, early cardiovascular training, and confidence with weight transfer. In a city where people want to get back to commuting on foot, training for local road races, or coaching from the sideline without limping, that bridge can matter.
What smart loading means
Patients often hear “progressive overload” and assume every session should be harder than the last. In ACL rehab, that mindset creates setbacks. Progress usually comes from choosing the right dose, then checking the knee's response over the next 24 hours.
A better standard is simple. The knee should tolerate the current level before you add depth, resistance, speed, or volume. If swelling rebounds, the exercise choice was too aggressive, the total workload was too high, or the recovery window was too short. For a plain-language explanation of the training concept, Strive Workout Log's guide is a helpful read.
Boston patients tend to do well when this phase is structured and practical. Strength sessions need to fit around commutes, class schedules, and long workdays. The plan still has to be demanding enough to rebuild the leg. That balance is what turns a decent recovery into one that holds up outside the clinic.
From The Clinic to The Esplanade Advanced Dynamic Training
This is the phase where patients start to feel athletic again. It's also the phase where people make expensive mistakes if they confuse confidence with readiness.
Running, jumping, decelerating, and cutting do not return because time passed. They return when strength, force absorption, coordination, and movement symmetry support them.
Why this phase is where good rehab separates itself
A lot of standard rehab programs do a decent job restoring range of motion and general strength. Fewer do a thorough job bridging the gap between clinic strength and the demands of sport.
That gap matters in Boston. A marathon trainee doesn't just need to jog. They need repeated impact tolerance. A soccer player at BU or Northeastern doesn't just need leg strength. They need deceleration, reactive control, and confidence in rotation. A recreational hockey player needs edge control and unpredictable force handling.
This phase should include objective criteria for entering a return-to-run progression, then a gradual climb through:
- Plyometrics with landing mechanics and force absorption
- Agility work such as lateral movement, acceleration, and deceleration
- Cutting and pivoting drills that rebuild rotational confidence
- Sport-specific patterns tied to your actual return goal
The role of neuromuscular training
Late-stage ACL rehab is not only about muscle size or gym numbers. It's also about retraining the body to coordinate force quickly and cleanly.
That is one reason prevention programs matter. The PEP program has been scientifically established to achieve an 88 percent injury reduction rate, and its neuromuscular focus mirrors the kind of movement quality work that shows up in mid-to-late ACL rehab according to Boston Children's Hospital's ACL program.
A strong single-leg squat does not guarantee a safe cut. Dynamic control has to be trained in dynamic conditions.
What Boston-specific progression can look like
The athlete who wants to get back to running along the Esplanade may start with controlled treadmill intervals, then outdoor flat running, then bridge work, then pace changes. The field sport athlete may move from line hops to controlled change-of-direction drills, then reaction-based drills, then non-contact practice.
This is also where performance testing becomes useful outside of formal return-to-sport clearance. Running analysis can help identify stride habits that unload one side. Golf-specific movement screens can matter for rotational athletes. A structured sport performance physical therapy program can be the bridge between basic rehab and the demands of real training.
Confidence has to be rebuilt too
Some patients look strong but still hesitate on a plant leg. Others say they trust the knee, then shorten stride, stiffen landings, or avoid rotation the moment speed goes up.
That doesn't mean they're failing. It means the last phase of rehab needs both physical exposure and psychological readiness. The answer usually isn't a speech. It's repeatable wins under the right level of challenge.
The Final Test Clearing You for Return to Sport
Return to sport is not a vibe. It is a clearance decision, and the decision should be defended with data.

The reason this matters is simple. Up to 1 in 5 people re-tear their ACL, but successfully completing a validated return-to-sport functional testing program can decrease reinjury risk by as much as 84% according to this Boston return-to-sport discussion. If an athlete skips the testing phase, they're often skipping the part most tied to long-term protection.
What the testing battery should answer
A real return-to-sport process should answer several questions, not just one.
- Strength question: Is the surgical leg producing enough force compared with the other side?
- Power question: Can the athlete hop, stick, and repeat without collapse or hesitation?
- Control question: Does movement stay clean when speed and fatigue rise?
- Sport question: Can the athlete tolerate the specific demands of soccer, skiing, rowing, hockey, or golf?
- Readiness question: Does the athlete trust the knee enough to move normally?
One study summarized in a clinical review found that athletes in supervised rehab had 76.6% return to the same level of sport participation, while the home-based group had lower return-to-sport performance overall, and both groups had 3.3% reinjury rates in that comparison. The same review also notes broader literature reporting roughly 81% return to some sport, 65% return to previous level, and 55% return to competitive sport, while one systematic review reported about 44% returned after an average of 41.5 months. Those details are discussed in the clinical review at PMC. The takeaway is not that return is impossible. It's that “back to sport” can mean very different things unless the criteria are specific.
What those tests often include
A Boston athlete nearing clearance should expect some combination of strength assessment, hop testing, landing analysis, change-of-direction testing, and sport-specific progression.
This video shows the kind of movement quality and control that matter late in rehab.
Why sport specificity matters
A rower on the Charles, a skier heading into winter, and a golfer preparing for a full rotational swing don't stress the knee in exactly the same way. The final stage should reflect that. Golf athletes may benefit from movement testing that looks at rotation, weight transfer, and control through the lead leg. Cutting-sport athletes need much more work in deceleration and directional change.
Clearance should answer, "Ready for what?" not just, "Ready compared to when?"
That distinction is where many reinjuries start. The athlete is ready for straight-line running, but not for chaos. Ready for drills, but not for unrestricted play. Ready for strength work, but not for fatigue and reaction.
Your ACL Recovery Partner in Boston
A strong ACL outcome usually comes from boring consistency, honest testing, and a plan that keeps changing as your knee changes. That's the genuine work. Not chasing milestones because a calendar says you should be there, and not stopping once pain is mostly gone.
For Boston patients, logistics are part of the clinical decision. If you're commuting through Back Bay, working in the Seaport, studying near Kenmore Square, or trying to fit rehab around a packed city schedule, access affects follow-through. So does having one clinician track the details of your gait, strength, swelling response, and return goals across the full arc of recovery.
That's where Joint Ventures Physical Therapy fits for many Greater Boston patients. The practice provides one-on-one physical therapy across Boston neighborhoods, along with specialty services that can matter during ACL recovery such as aquatic therapy, running performance, dry needling, concussion baseline screening, and Titleist evaluations for golf-specific return planning. For deeper educational content on ligament healing, sports rehab science, and injury recovery topics that go beyond local care logistics, visit Highbar Health.
If you're looking for ACL recovery physical therapy Boston athletes and active adults can stick with, the right next step is simple. Get evaluated early, use objective milestones, and treat return to sport as something you earn through testing rather than assume with time.
If you're ready to start ACL recovery physical therapy Boston patients can fit into real life, book an evaluation with Joint Ventures Physical Therapy. With locations across Greater Boston, including Back Bay, Kenmore Square, Fort Point/Seaport, and Downtown, the team helps athletes, runners, students, and active professionals move from early rehab to return-to-sport testing with one-on-one care.


