You leave a doctor’s appointment with one simple instruction: “Start therapy.” Then the immediate question hits. What kind of therapy?
If you’re searching for what is occupational therapy vs physical therapy, you’re not confused because you missed something obvious. The terms overlap in conversation, many referrals are vague, and a lot of online explanations flatten the distinction into something too simple to be useful.
That matters, because choosing the right starting point can save time, frustration, and unnecessary bouncing between providers.
In practice, the difference isn’t just “PT helps you move” and “OT helps you use your hands.” Sometimes that’s directionally true. It’s also incomplete. A runner with pelvic floor symptoms may need movement retraining and daily activity strategies. A patient with jaw pain may need postural work, breathing mechanics, and habit changes around eating, speaking, and desk setup. A hand injury can limit grip strength, but the ultimate goal may be returning to keyboard work, cooking, lifting a child, or getting back to climbing.
The best rehab plan starts with the question: What are you trying to get back to doing?
Starting Your Recovery Journey With Confidence
Individuals often begin their journey with a shared experience. They have pain, stiffness, weakness, dizziness, pelvic floor symptoms, or trouble doing something that used to feel automatic. Then they hear the words “physical therapy” or “occupational therapy” and aren’t sure which one fits.
That uncertainty is normal.
Some diagnoses point clearly in one direction. A fresh ankle sprain usually belongs with a physical therapist. Difficulty getting dressed after a hand injury often belongs with an occupational therapist. But many real cases sit in the middle, especially when pain, movement, work demands, sports, parenting, and daily routines all affect each other.
What usually helps first
Start with your goal, not the label.
Ask yourself:
- Are you trying to move better? Think walking, running, lifting, turning your head, climbing stairs, changing direction, or getting through a workout without pain.
- Are you trying to function better in daily life? Think getting dressed, typing, cooking, gripping, caring for a baby, managing fatigue, or returning to work tasks.
- Are both problems happening at once? That’s common. It often means you need a team that can coordinate care instead of working in separate silos.
Practical rule: If your biggest barrier is body mechanics, pain with movement, or loss of mobility, PT is often the best place to start. If your biggest barrier is doing meaningful daily tasks safely and efficiently, OT may be the better first call.
Access also matters more than people think. Clear communication, easy scheduling, and usable digital systems shape whether patients begin care and stick with it. If you’re interested in the patient side of healthcare accessibility, that resource does a good job explaining why access isn’t only about ramps and parking.
A first visit should reduce confusion, not add to it. If you’re getting ready for an evaluation, this guide on how to prepare for your first physical therapy appointment can help you walk in with better questions and clearer expectations.
The Guiding Philosophies of PT and OT
Physical therapy and occupational therapy both help people recover. They just start from different clinical priorities.
Physical therapy asks, in essence, “How do we restore the body’s capacity to move well?” Occupational therapy asks, “How do we help this person participate in the activities that make up life?”
Those are not competing ideas. They’re different lenses.

What physical therapy is trying to restore
PT is built around movement quality, mobility, strength, pain reduction, and physical performance.
That includes walking, squatting, getting up from the floor, returning to running, recovering after surgery, improving balance, and rebuilding tolerance for force and load. PT often focuses on gross motor function. Larger movement systems. Joints. Muscles. gait. coordination.
A helpful way to think about it is this: PT often works on the body capacities that make action possible.
If you want to understand a clinic model that includes this kind of movement-based care alongside specialized rehab, it helps to look at a dedicated occupational therapy service page too, because the overlap becomes clearer when both disciplines are offered intentionally.
What occupational therapy is trying to restore
OT centers on participation in daily life.
In rehab, “occupation” doesn’t mean only employment. It means the activities that fill your day and give it structure or meaning. Dressing. Grooming. Meal prep. Parenting tasks. School. Keyboard use. Fine motor work. Sensory regulation. Workplace demands. Adaptive strategies when your body isn’t ready to do things the old way.
OT often steps in when the question isn’t only “Can you move this joint?” but “Can you do what your life requires?”
A PT may help you regain the strength and mobility to climb stairs. An OT may help you carry laundry, manage hand use on the railing, and problem-solve the task safely when pain or weakness changes your routine.
Why both fields continue to grow
This distinction matters because demand for both professions is strong. In the United States, there are approximately 258,200 physical therapists and 143,300 occupational therapists, with projected growth of 15% for PTs and 11% to 14% for OTs in the relevant BLS windows cited here by Spry PT.
That growth reflects the needs clinicians see every day. People are living longer, staying active later in life, returning to sport after injury, navigating chronic pain, and expecting rehab to help them function, not just feel slightly better.
A Side-by-Side Comparison of Physical and Occupational Therapy
When patients ask for the clearest answer to what is occupational therapy vs physical therapy, I usually tell them to compare four things: training, treatment focus, clinical tools, and end goals.
That framework is simple enough to remember and detailed enough to help.
| Criteria | Physical Therapy (PT) | Occupational Therapy (OT) |
|---|---|---|
| Core question | How do we improve movement, strength, mobility, and pain? | How do we improve function in daily life and meaningful activities? |
| Typical movement lens | Gross motor patterns, gait, balance, joint mechanics, tissue loading | Fine motor control, task performance, hand use, sensory processing, activity adaptation |
| Common patient goals | Walk without pain, return to sport, rebuild after surgery, improve balance | Dress independently, work comfortably, cook safely, improve hand function, manage daily routines |
| Assessment style | Body mechanics, mobility, strength, tolerance to movement, balance | Functional task analysis, hand use, coordination, environmental setup, daily activity barriers |
| Typical interventions | Therapeutic exercise, manual therapy, mobility work, gait training, neuromuscular retraining | Task practice, activity modification, adaptive equipment, ergonomic strategies, fine motor training |
| Best first fit | Pain or limitation driven mainly by movement loss or physical performance deficits | Difficulty completing daily tasks efficiently, safely, or independently |
| Where they overlap | Return to life, work, parenting, sport, and independence | Return to life, work, parenting, sport, and independence |
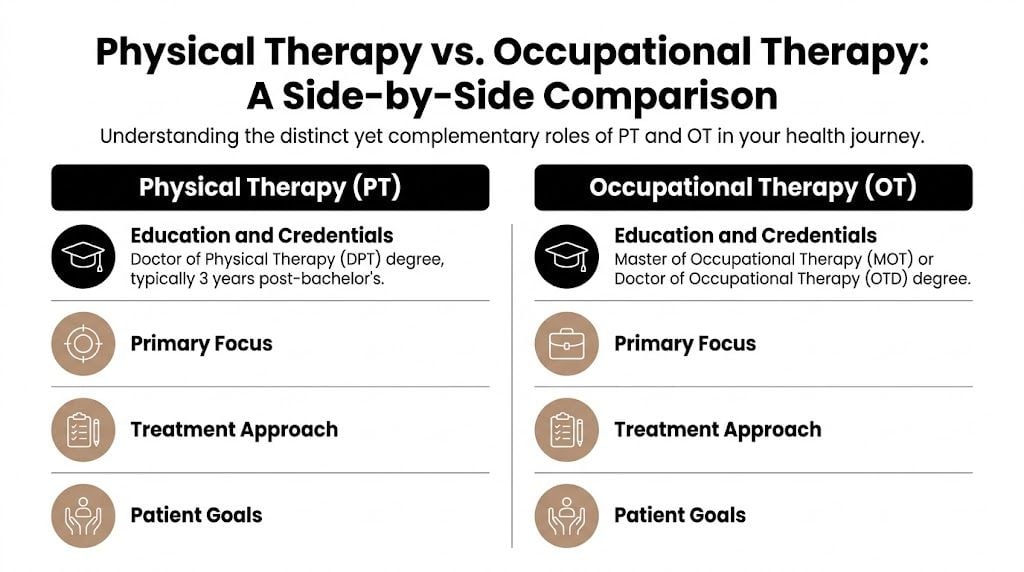
Education and credentials
Physical therapists complete doctoral-level professional training. Occupational therapists enter practice through graduate-level OT education. In day-to-day patient care, what matters most isn’t academic title alone. It’s how that training shapes clinical thinking.
PT education leans heavily into biomechanics, movement analysis, exercise prescription, and restoration of physical capacity. OT education emphasizes function, task analysis, adaptation, and the interaction between body limitations and real-world demands.
If you're curious about the broader educational pathway to become a physiotherapist, that overview is useful for career context, though patients benefit most from understanding how training shows up in treatment decisions.
Primary treatment focus
The difference becomes practical here.
A physical therapist often tracks change in terms of joint motion, strength, balance, gait, load tolerance, and movement quality. An occupational therapist often tracks change in terms of what the person can do with those abilities in daily life.
A PT may look at whether your shoulder moves overhead without compensation. An OT may look at whether you can reach a shelf, wash your hair, or tolerate repeated reaching during work.
A PT may rebuild lower body force production after surgery. An OT may help translate recovery into job demands, home routines, or sport-specific hand use.
The tools each one uses
PTs and OTs both use exercise. Both educate. Both reassess. But they usually apply those tools differently.
According to Mid America Orthopedics, physical therapy often targets biomechanical metrics such as improving range of motion by 10% to 20% in 4 to 6 weeks through manual mobilization, while occupational therapy uses standardized tests like the Nine-Hole Peg Test, with a normative score of under 20 seconds for adults, to benchmark fine motor dexterity required for daily tasks.
What PT often looks like in the clinic
A PT plan commonly includes:
- Manual therapy: Joint mobilization, soft tissue work, and hands-on techniques to improve mobility or reduce pain.
- Therapeutic exercise: Strengthening, endurance, and graded loading based on tissue irritability and patient goals.
- Neuromuscular retraining: Teaching the body to coordinate movement better, not just move more.
- Gait and balance work: Especially important after surgery, concussion, vestibular problems, or lower extremity injury.
A person recovering from knee surgery may spend time on knee extension, quad activation, stair mechanics, deceleration control, and return-to-run progressions. The sessions are less about “feeling worked on” and more about restoring the physical prerequisites for normal movement.
You can see how this movement-first approach fits within a broader physical therapy model that addresses orthopedic care, sports rehab, and more complex performance issues.
What OT often looks like in the clinic
An OT plan often includes:
- Task-specific practice: Rehearsing the exact activities that matter, not just isolated motions.
- Fine motor training: Dexterity, in-hand manipulation, pinch, grip, coordination, and precision.
- Adaptive strategies: Changing how a task is done when pain, weakness, sensory issues, or healing limits the usual method.
- Environmental and ergonomic changes: Adjusting the setup at home, school, or work so the body isn’t fighting the task all day.
A patient with a hand injury may not only need stronger grip. They may need to hold a pan, open a jar, type for sustained periods, or manage buttons and zippers without flare-ups. OT tends to stay close to those real tasks.
Clinical shortcut: PT often rebuilds the engine. OT often makes sure the engine works in traffic, on hills, and in real life.
Ultimate goals and outcomes
Patients sometimes assume PT is more medical and OT is more practical. That split isn’t accurate.
Both are practical. Both are medical. Both should produce measurable change.
The difference is where success is centered.
For PT, success often sounds like this:
- Pain is lower with walking, lifting, turning, or training.
- The joint moves better.
- The patient can tolerate higher loads.
- Balance and mobility have improved enough to return to a desired activity.
For OT, success often sounds like this:
- The person can dress, cook, write, carry, type, or parent with less difficulty.
- A work task no longer triggers symptoms so quickly.
- Fine motor control is more efficient.
- The patient has a strategy that makes daily life sustainable, not just possible for one day.
What doesn’t work
The wrong referral logic causes problems.
These are common mistakes:
- Referring only by body part: “Arm equals OT, leg equals PT” misses pelvic floor, TMJ, concussion, and many upper quarter problems.
- Treating pain without asking about function: A patient may report lower pain but still be unable to work, train, or care for family.
- Waiting too long to coordinate: When a person clearly needs both movement restoration and task adaptation, delayed collaboration slows progress.
Where the Lines Blur The Power of Integrated Care
The most useful answer to what is occupational therapy vs physical therapy is also the one many websites skip. The lines blur all the time.
That isn’t a problem. It’s often the reason patients get better.
Complex conditions don’t behave neatly
Pelvic floor dysfunction, TMJ pain, vestibular disorders, persistent post-surgical symptoms, chronic pain, and high-level return-to-sport cases rarely fit a one-discipline story.
A postpartum runner may have pelvic floor symptoms, hip weakness, breath-holding patterns, lifting strain, and difficulty returning to exercise with confidence. A patient with TMJ dysfunction may also have neck stiffness, poor ribcage expansion, stress-related clenching, and trouble eating certain foods. A desk worker with dizziness may need balance retraining, visual tolerance work, and practical strategies for screens, commuting, and work pacing.
If you force those people into a narrow lane, progress usually stalls.
What integrated care changes
Integrated care means the treatment plan follows the patient’s problem instead of protecting professional turf.
A PT might address mobility restrictions, loading tolerance, posture, gait, breathing mechanics, and force generation. An OT might address task setup, habit patterns, ergonomic demands, feeding strategies, hand use, sensory triggers, and how symptoms affect work or self-care.
Those are complementary moves.
According to a UCLA Med School article, a 2025 study highlighted that 68% of pelvic floor patients benefit from hybrid PT-OT models, with functional outcomes improving by 40% compared to siloed care. The article notes this approach helps address referral confusion and delayed recovery.
That finding fits what many clinicians have observed for years. People with layered problems usually need layered care.
When progress plateaus, the issue often isn’t patient motivation. It’s that the plan is too narrow for the problem.
What collaborative treatment looks like
In a coordinated plan, clinicians don’t duplicate each other. They solve different parts of the same puzzle.
For example:
- Pelvic floor rehab: PT may work on muscle coordination, pressure management, and return-to-impact progression. OT may work on bladder routines, self-care logistics, activity pacing, and return to daily roles.
- TMJ care: PT may treat cervical mobility, jaw mechanics, posture, and breathing. OT may address chewing habits, desk setup, symptom management during work, and self-regulation strategies.
- Sports rehab: PT may handle force production, landing mechanics, and conditioning progressions. OT may address upper extremity control, equipment interaction, hand use, or return-to-school and work routines around training.
The win isn’t just “more providers.” The win is less fragmentation.
Real Patient Scenarios How PT and OT Help
Abstract definitions only go so far. Patients usually understand the difference once they can see it in a real recovery process.

The athlete returning after ACL surgery
This patient usually starts with obvious PT needs.
The knee is stiff. Strength is down. Confidence is shaky. Running and cutting feel far away. Early priorities include restoring motion, reducing swelling, rebuilding quadriceps function, and retraining gait and single-leg control.
PT drives that process because the body has to regain its physical capacity before sport becomes realistic.
But the athlete’s life isn’t only rehab exercises.
If the patient is also struggling with school or work setup during recovery, carrying gear, managing daily tasks while protecting the surgical leg, or returning to upper extremity-intensive sport tasks, OT may become relevant. The same is true if a brace, crutches, or post-operative limitations turn ordinary routines into barriers.
The key trade-off is timing. Too much sport-specific ambition before movement quality returns usually backfires. On the other hand, waiting too long to reconnect rehab to the patient’s actual routines can make progress feel abstract and discouraging.
The postpartum runner with pelvic floor symptoms
This is one of the clearest examples of why siloed care fails.
The patient may report leaking with impact, pelvic heaviness, hip or back pain, and fear around returning to running, lifting, or core work. A purely fitness-based plan often misses the pelvic floor coordination piece. A purely symptom-based plan may calm things down but never bridge back to real movement demands.
PT often leads the physical side. Breathing strategy, pressure management, strength, impact preparation, and graded return to exercise all matter.
OT can be just as important once the question becomes: how does this person manage daily life while recovering?
That may include:
- Infant care routines: Repetitive lifting, carrying, feeding positions, and floor transfers.
- Bladder and habit patterns: Daily routines that unintentionally increase symptoms.
- Return to role demands: Work, commuting, exercise scheduling, and home task pacing.
- Environmental setup: Stroller use, nursery layout, seating, and strategies that reduce unnecessary strain.
What doesn’t work here is pretending the patient has to choose between “fixing the muscles” and “learning to live around it.” Good rehab does both.
Patients often feel relieved when someone finally connects symptom reduction to the activities they actually want back.
The office worker with TMJ pain and headaches
TMJ dysfunction is rarely just a jaw problem.
A patient may come in with pain while chewing, clicking, headaches, neck tension, clenching, poor sleep, and a workday built around screens and stress. If care focuses only on the jaw joint itself, progress tends to be partial.
PT can address cervical spine stiffness, postural loading, ribcage mechanics, breathing pattern issues, and jaw mobility. Those drivers matter because the jaw doesn’t work in isolation from the neck and upper quarter.
OT brings a different level of detail to the day.
An OT may look at:
- Meal patterns and chewing demands
- Workstation setup and symptom triggers
- Oral habits during concentration
- Strategies for pacing long speaking or meeting days
- Behavioral routines that keep the jaw overloaded
The trade-off in TMJ rehab is that some patients want only manual treatment. Hands-on care can help. But if no one addresses stress habits, positioning, or daytime behaviors, symptoms often return quickly.
The patient with a hand and upper extremity injury
Many people first understand OT clearly at this stage.
A hand or wrist injury affects everything. Opening containers, typing, carrying groceries, gripping a steering wheel, lifting a child, meal prep, sports equipment, handwriting. Small losses create big friction.
OT is often the lead discipline because fine motor control, splinting, dexterity, grip use, swelling management, and task adaptation all sit close to occupational therapy’s core strengths.
But PT may still matter if the problem travels up the chain.
Shoulder weakness, scapular control deficits, neck tension, postural strain, or altered upper quarter mechanics can all keep the hand from recovering smoothly. A patient may protect the wrist so aggressively that they create secondary shoulder or neck pain. In those cases, PT and OT work best when they coordinate rather than handing the patient back and forth.
The patient with dizziness who also can’t function normally
Vestibular complaints are another area where labels get blurry.
A patient with vertigo, motion sensitivity, or imbalance often needs PT for gaze stabilization, balance retraining, gait confidence, and movement exposure. Those are classic movement-system problems.
But the patient may also be struggling to shop, commute, use screens, read, cook, or tolerate busy visual environments. OT can help translate progress into daily tasks and reduce the gap between “I can do this drill in clinic” and “I can get through my day.”
That distinction matters because many patients improve in treatment sessions before they improve in life. The second step needs its own clinical attention.
A simple way to think about the scenarios
Across all of these examples, the pattern is consistent:
- PT restores physical capacity
- OT restores functional participation
- Complex patients often need both
That’s why simplistic explanations create bad expectations. Individuals typically aren’t trying to improve a body part in isolation. They’re trying to get back to a life.
How to Choose the Right Therapy for Your Goals
The fastest way to choose well is to stop asking, “Which profession is better?” and start asking, “What problem is getting in my way most right now?”

Start with the activity you want back
If your answer sounds like “I want to walk, run, squat, lift, turn my head, get stronger, or stop hurting when I move,” start with PT.
If your answer sounds like “I want to dress myself, type without symptoms, cook, care for my baby, manage work tasks, or use my hand normally again,” start with OT.
If your answer includes both. Which it often does. Find a setting that can evaluate the overlap instead of forcing you into an artificial category.
A few practical if-then rules
- If pain shows up mainly during movement or exercise, PT is usually the better first referral.
- If the biggest issue is completing daily tasks safely or efficiently, OT often makes more sense.
- If you have a pelvic floor, TMJ, vestibular, or post-surgical problem that affects both movement and routine life, ask for coordinated care.
- If your diagnosis is clear but your goal is complicated, choose based on the goal.
A runner with pelvic pain doesn’t need a generic “core program.” A desk worker with jaw pain doesn’t need only a mouthguard discussion. A hand injury patient doesn’t need strength testing alone if they still can’t function through a workday.
Questions worth asking before you start
Bring these to the first conversation:
- What will you measure first?
- How will treatment connect to my actual goals?
- If my problem overlaps both PT and OT, how is that handled?
- What should I expect to work on at home?
- What would tell you I need a different or more integrated approach?
A good clinician won’t be defensive about those questions. They’ll welcome them.
Here’s a short video that can help frame the decision from a patient perspective.
What the right choice should feel like
The right starting point should make your plan clearer within the first visit or two.
You should understand:
- What the clinician thinks is driving the problem
- What the immediate priorities are
- How progress will be judged
- Whether another discipline should be involved
Good rehab doesn’t just tell you what hurts. It tells you what the plan is, why it fits, and how it gets you back to your own life.
Your Partners in Recovery at Joint Ventures
The difference between PT and OT becomes much easier once you anchor it to a real goal. PT helps restore the physical capacity to move. OT helps restore the ability to function through daily life. For many patients, especially those dealing with pelvic floor issues, TMJ dysfunction, sports rehab, dizziness, or upper extremity problems, the best answer isn’t one or the other. It’s the right blend at the right time.
That’s where a 1-on-1 model matters.
When a clinician has uninterrupted time to listen, evaluate, and adjust, it’s easier to catch the details that change a plan. The sport that matters. The work task that keeps flaring symptoms. The postpartum routine no one asked about. The jaw habit tied to long screen days. The reason a patient is “doing better” on paper but still not back to living normally.
Joint Ventures offers both physical and occupational therapy under one roof, with specialists who understand these overlaps and build care around the person, not just the diagnosis.
If you’re trying to figure out whether PT, OT, or a coordinated plan is the right fit, Joint Ventures Physical Therapy can help you make that decision with clarity. Reach out for guidance, ask questions, and start with a plan built around your real goals.


