Boston runners are good at pushing through discomfort. That trait helps on long winter builds, hill repeats, and windy Charles River runs. It also gets people in trouble.
A lot of runners wait too long to get help. They hope the knee will “warm up,” the Achilles will settle after a down week, or the hip pain will disappear once work gets less busy. Then they miss key training, lose confidence, and start guessing. If that’s where you are right now, you’re not behind. You just need a better plan.
Your Guide to Navigating Running Injuries in Boston
You sign up for a race, stack a few solid weeks, and then something starts talking back. Maybe it’s the outer knee on descents. Maybe it’s the calf that tightens every time you push the pace. Maybe it’s a deep ache that shows up after your run and lingers on the stairs the next morning.
In Boston, that kind of interruption hits harder. Running is part of the city’s rhythm. People train before work along the Esplanade, squeeze in miles around Back Bay, and build toward spring with the Boston Marathon in mind even if they’ll never toe that start line. When running gets taken away, it doesn’t feel like “just an injury.” It feels like your routine, stress relief, and identity all took a hit at once.

That demand is visible at the biggest race in town. The Boston Marathon mobilizes approximately 100 physical therapists at the finish line, and the 2024 event drew about 30,000 athletes from more than 100 countries, according to Northeastern’s reporting on Boston Marathon medical support. A city that supports that many runners needs clinicians who understand running injuries at a high level.
What most injured runners want
Active individuals don’t want a lecture about stopping all activity. They want answers to practical questions:
- Can I keep running at all
- What is causing this
- How long until I’m back to normal
- What do I need to change so it doesn’t come back
Those are fair questions. They deserve better than “rest and stretch.”
You can’t train confidently when you don’t know whether each run is helping, hurting, or just delaying the real fix.
Boston runners also tend to be curious and disciplined. If that’s you, it helps to pair your rehab with smart habits outside the clinic. A simple resource on how to prevent running injuries can complement the more individualized work you do in PT.
A good running injury plan should do two things at once. It should calm the current problem down, and it should rebuild the movement and loading capacity that let you train hard again.
Why Generic Physical Therapy Fails Dedicated Runners
A runner comes in with knee pain and gets clamshells, bridges, heat, and a printout. That approach isn’t useless. It’s just often incomplete.
Running places repeated demands on tissue, timing, force absorption, and coordination. If treatment only chases the painful area, the underlying cause often stays in place. The knee hurts, but the issue may be stride mechanics, pelvic control, ankle mobility, training progression, or how your body handles impact when fatigue sets in.
The problem with symptom-only rehab
Generic PT often breaks down in a few predictable ways:
- It treats location, not cause. Pain at the shin, knee, or Achilles becomes the whole story, even when the source sits elsewhere in the chain.
- It ignores running load. Mileage, workouts, hills, shoes, and recent training changes matter. If nobody asks, the plan is missing part of the picture.
- It relies on full rest for too long. Some runners need unloading. Others need modified loading, not complete shutdown.
- It never watches you run. For a runner, that’s a major omission.
Boston has enough running-specific demand that specialized centers exist just for the tougher cases. The Spaulding National Running Center is built around complex running injuries that haven’t improved with standard PT. That tells you something important. A meaningful subset of runners need more than conventional orthopedic care.
Why Boston runners need a more specific lens
Boston isn’t a flat, controlled treadmill-only environment. Local runners deal with hills, brick and uneven surfaces, winter stiffness, spring race builds, and the temptation to push through because everyone around them seems to be training too.
Here’s where generic advice usually misses:
| Common advice | What happens | Better approach |
|---|---|---|
| Rest until pain is gone | Fitness drops, confidence drops, root issue may remain | Match loading to tissue tolerance and monitor response |
| Strengthen the painful area | Helpful, but often too narrow | Strength plus gait, mobility, and training review |
| Return when it “feels okay” | Many runners come back too fast | Use objective benchmarks before progression |
Clinical reality: if rehab never gets specific enough to running, a dedicated runner often finishes PT feeling “better” but not actually ready for training.
Signs you need running-specific care
You’ll usually recognize the mismatch quickly. Watch for these signs:
Nobody asks about your race goals or weekly schedule.
A Boston Marathon hopeful and a casual jogger don’t need the same plan.Your sessions focus on pain relief, not return to performance.
Relief matters. It just can’t be the endpoint.You’ve had PT before for the same issue.
Repeating the same formula rarely changes the result.
Runners don’t need magic. They need a clinician who understands the trade-offs between calming symptoms now and preparing the body for the next training block.
The Comprehensive Running Assessment You Deserve
You do not need another rushed visit where someone pokes the sore spot, hands you a printout, and tells you to take a break from running. Boston runners usually come in with a deadline. A fall marathon, a spring BAA attempt, a return after having a baby, or the frustration of the same pain showing up every training cycle. The assessment has to explain why the problem started, what is keeping it around, and what will let you train again without guessing.
The first step is a detailed history. That means training volume, recent pace changes, hill work, long-run structure, shoe rotation, sleep, recovery, prior injuries, and what your week looks like outside running. It also means listening for patterns that matter in harder cases. Postpartum runners may be dealing with pelvic floor symptoms, abdominal wall changes, or a sharp drop in strength and sleep. Runners with repeat injuries often have a load-management issue layered on top of a movement problem, not just a painful tissue.
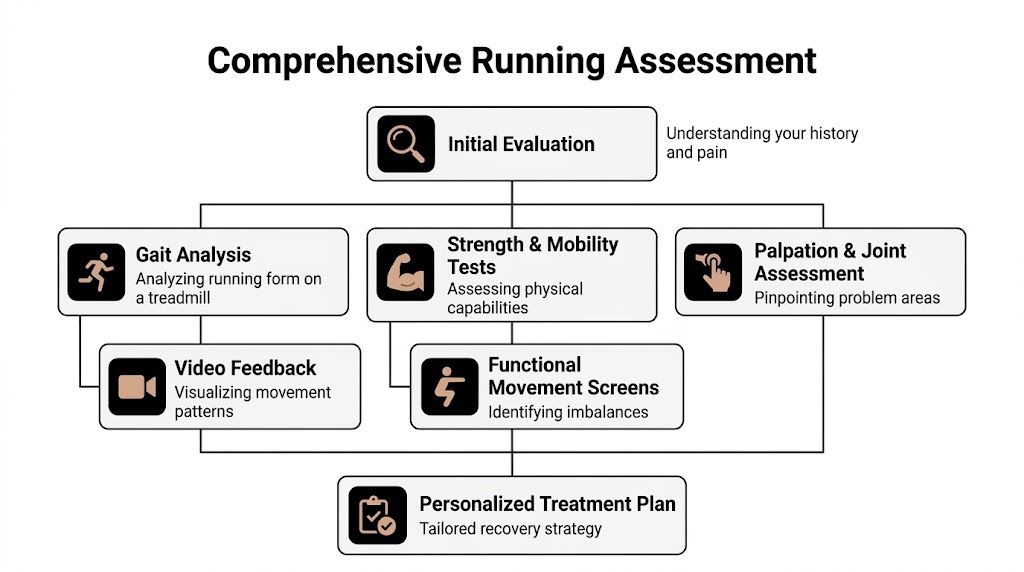
What a serious evaluation includes
After the history, the exam should test the pieces that drive running performance and running pain:
- Single-leg movement quality to see how you control load at the foot, knee, hip, and trunk
- Strength testing for muscle groups that need to absorb force and keep form from breaking down
- Mobility assessment at the ankle, hip, foot, and thoracic spine
- Hands-on exam to sort out tissue irritability, stiffness, and symptom response
- Running analysis on a treadmill or overground to see what changes once you start moving at real running speeds
Running analysis is often the missing piece.
According to Spaulding’s running clinic information, expert running evaluations use instrumented treadmill assessments with video gait analysis and capture over 60 biomechanical data points. That same source notes that faulty mechanics are causally linked to 70 to 80 percent of running injuries, and targeted gait retraining can reduce reinjury risk by up to 62 percent.
That does not mean every runner needs a lab-style setup or that form changes solve everything. It means good rehab should include objective observation of how you run, especially if you have had symptoms more than once or your pain only shows up at certain distances or paces.
A useful gait review looks at cadence, pelvic control, trunk position, foot strike pattern, asymmetry, and what happens as fatigue builds. Those findings shape treatment. A runner with Achilles pain may need calf capacity, ankle stiffness work, and a temporary change in hill exposure. A runner with the same pain after returning postpartum may also need pelvic stability work and a slower progression plan because tissue tolerance is different.
At Joint Ventures, a running form assessment with video analysis and corrective exercise guidance helps connect those details to a plan you can use in training. You should leave with clear feedback, specific benchmarks, and a treatment plan tied to what the assessment found.
Advanced Treatments to Accelerate Your Recovery
Strength and loading still do most of the heavy lifting in rehab. Advanced tools matter when they support that work, not when they replace it.
That distinction matters because runners often get sold passive care when what they really need is a sharper progression. The right adjunct can speed things up. The wrong one just eats time.

Where dry needling helps
For runners, trigger points and stubborn muscle tone can block progress. You keep doing the exercises, but the calf stays guarded, the lateral quad keeps grabbing, or the glute never feels like it turns on correctly.
That’s where dry needling can be useful. It’s a targeted technique that can reduce excessive resting tone and make it easier to move, strengthen, and retrain a pattern that’s been stuck.
The Ripple Boston guide to physical therapy in Boston reports that dry needling can decrease muscle resting tone by 25 to 40 percent and has been linked in randomized controlled trials to a 40 percent faster return-to-run compared with manual therapy alone.
That doesn’t mean every runner needs needles. It means some runners respond well when muscle guarding is one of the factors keeping them from loading effectively.
Where BFR changes the game
Blood Flow Restriction, or BFR, is one of the most practical tools for runners who need to build strength without piling stress onto an irritable joint or tendon.
That matters when:
- Patellar tendon pain limits heavier quad work
- Calf or Achilles issues make full loading hard early on
- Post-injury weakness is obvious, but traditional strength work flares symptoms
- Return-to-run prep requires rebuilding tissue capacity before mileage climbs
The same Boston resource notes that BFR can support strength gains with low joint stress. For runners, that trade-off is often exactly what’s needed in early and mid-stage rehab.
What works and what doesn’t
A few practical distinctions help:
| Treatment choice | Works best when | Usually falls short when |
|---|---|---|
| Dry needling | Tone, pain, and guarding are limiting exercise quality | It’s used as a stand-alone fix |
| BFR | You need strength adaptation with lower mechanical stress | No one is tracking progression or exercise form |
| Manual therapy | You need short-term mobility or symptom relief | It replaces strength and movement retraining |
If you’re looking into hands-on care, this overview of manual physical therapy gives a useful frame for how these tools should fit into a larger plan.
The best advanced treatment is the one that makes your next exercise session more productive, not the one that feels most impressive during the visit.
For Boston runners, that matters. You need treatment that helps you absorb load on the hills, tolerate volume, and return to a training plan with fewer setbacks.
A Specialized Path for Postpartum Runners in Boston
A lot of postpartum runners hear a version of the same message. Wait a bit, ease back in, and listen to your body. The problem is that this advice is too vague for someone trying to return to running safely.
Postpartum recovery changes breathing mechanics, abdominal control, pelvic floor function, hip strength, and impact tolerance. If a runner leaks with strides, feels pelvic heaviness after a run, or develops new low back, hip, or pubic region discomfort, that’s not something to ignore and “hope improves with time.”
Why this group needs integrated care
The gap in local content is real. According to The Rx Movement’s review of the topic, 65% of runners experience annual injuries, and postpartum women face compounded risks, with up to 66% reporting pelvic floor dysfunction. That same source notes that Boston-specific running rehab content largely overlooks the integration of pelvic floor therapy with return-to-run care.
That gap matters because postpartum runners often get split into two separate categories:
- orthopedic rehab for pain
- pelvic floor therapy for leaking, pressure, or prolapse symptoms
In practice, those problems often overlap. A runner doesn’t move in orthopedic pieces and pelvic health pieces. She runs as one system.
What integrated rehab looks like
A more useful postpartum running plan looks at:
- Breathing and pressure management during impact and exertion
- Core and pelvic floor coordination under running-specific demand
- Single-leg control because running is repeated single-leg loading
- Hip and trunk strength for force transfer and control
- Return-to-run progression based on symptoms, not just calendar time
Some postpartum runners need pelvic floor downtraining before they need more strengthening. Others need strength, loading, and confidence because they’ve become overly protective. The right answer depends on the individual presentation.
A postpartum runner shouldn’t have to choose between seeing someone who understands sport and someone who understands pelvic health.
That’s why dual-skill care matters. A clinician who can connect leakage, heaviness, low back pain, and running mechanics is in a better position to build a realistic path back.
If that’s your situation, this article on pelvic floor therapy after pregnancy is a useful starting point.
What not to accept
Postpartum runners should be cautious about advice that sounds simple but skips the hard parts:
“You’re cleared, so just start slow.”
Medical clearance and running readiness are not the same thing.“If it doesn’t hurt, it’s fine.”
Pelvic floor symptoms don’t always show up as pain.“Do Kegels and see how it goes.”
Some people need relaxation, coordination, and whole-body loading work, not more squeezing.
Boston has a deep running culture. Postpartum runners deserve to be treated as runners, with all the nuance that requires.
Building Your Confident Return to Running Plan
The question every injured runner asks is simple. “When can I run again?”
The honest answer is that return to running should be criteria-based, not based on wishful thinking or a generic timeline. That matters because prior injury is the top risk factor for getting hurt again, and Elliott Physical Therapy’s runner therapy page cites 40 to 70 percent re-injury rates within 12 months. The same source notes that evidence-based, graded return-to-run protocols can cut that recidivism rate by 28 percent.

What readiness actually means
Most runners are not held back by motivation. They’re held back by either underprepared tissue or a plan that progresses too fast.
Before building mileage, I want a runner thinking about three buckets:
Symptoms
Are pain and post-run irritability predictable, mild, and settling appropriately?Capacity
Can the involved tissues tolerate strength work, walking, stairs, and single-leg tasks without a spike afterward?Control
Can you manage the movement quality needed for repeated impact?
A strong return-to-run plan doesn’t remove all discomfort from the process. It gives you a framework for deciding what level of discomfort is acceptable and what signals mean you need to back off.
How progression usually works
Most successful plans start with controlled exposure. That often means walk-run intervals before continuous running, flatter routes before hills, and restraint before speed work.
A practical progression usually includes:
| Phase | Focus | What the runner is proving |
|---|---|---|
| Early re-entry | Walk-run intervals | Impact is tolerated without a symptom spike |
| Volume build | More continuous easy running | Tissue handles repeated loading |
| Terrain and pace | Hills, strides, moderate efforts | Mechanics and capacity hold under higher demand |
| Full training | Normal weekly structure | Runner can recover between sessions |
That structure matters because many Boston runners jump from “I can jog a little” to “I’m basically back.” That gap is where setbacks happen.
Here’s a short visual that captures the idea of controlled progression:
What your PT should adjust in real time
A good return plan isn’t rigid. It responds to what your body shows.
Decision rule: if a progression looks good on paper but your body doesn’t handle it well, the paper loses.
The useful adjustments often involve surface, frequency, stride cues, footwear decisions, strength dosage, and what else is happening in your week. A runner commuting on foot, carrying a tired calf from standing all day, and sleeping poorly may need a different progression than the training log alone suggests.
Confidence comes from evidence. Not from forcing it.
How to Choose Your Running Physical Therapist in Boston
You book a PT appointment because your knee has been barking since the Chestnut Hill hills, or your pelvic floor symptoms started the week you tried to build mileage again after delivery. You do not need a generic exercise sheet. You need someone who can figure out why running keeps provoking the problem, what your body is tolerating right now, and how to get you back to training without repeating the same cycle.
That is the standard to use when choosing a running physical therapist in Boston.
A strong fit starts with focus. Some orthopedic PTs treat a wide range of issues well, but dedicated runners do better when the clinician regularly works with training loads, race calendars, gait changes, postpartum return, and the frustration of re-injury. If your goal is the Boston Marathon, a fall half, or even getting through a week of easy runs without pain, your PT should treat that goal as part of the case, not as background information.
What to look for
Use a short filter before you book.
One-on-one care
Running injuries usually require observation, strength testing, load planning, and follow-up adjustments. That works better with direct time from the same clinician.A real running assessment
A clinic should be able to watch you run and connect what they see to your symptoms, training history, strength, mobility, and recovery habits.Experience with performance-minded runners
Pain at rest is only part of the picture. Boston runners often care about hills, pace changes, long-run tolerance, and whether a plan holds up under real training demands.Skill with complex cases
Repeated calf strains, stubborn tendon pain, postpartum symptoms, and overlapping pelvic health and orthopedic issues need more than standard rehab templates.Useful treatment options when they fit the problem
Dry needling, blood flow restriction training, pelvic floor therapy, vestibular and balance care, orthotic support, and strength-based rehab can all have a place. The value is not having every tool. The value is knowing when to use each one and when not to.A convenient location
Consistency matters more than good intentions. If visits do not fit your workday, commute, or training schedule, adherence usually drops.
Questions worth asking before you schedule
Good clinics should answer these clearly.
Will I see the same clinician each visit?
Continuity helps when your plan needs small changes based on symptoms, recovery, and training response.Do you assess running mechanics directly?
Saying a clinic treats runners is different from studying how you load, move, and compensate while running.Do you work with postpartum runners and repeat injuries?
Boston runners are not one group. A runner returning after pregnancy needs a different lens than a runner chasing a PR after three rounds of Achilles pain.What treatment options are available in-house?
If your case may benefit from dry needling, BFR, pelvic floor therapy, or balance work, it helps when the clinic can provide that care without sending you elsewhere.Is the clinic convenient enough for regular follow-through?
Back Bay, Kenmore Square, Fort Point and Seaport, Downtown Boston, Brookline, and Allston access can matter a lot once rehab has to coexist with work, family life, and training.
What separates a stronger local option
Boston running has its own demands. Cold weather training changes tissue tolerance. Sidewalks, hills, river paths, and marathon build-ups create patterns that local clinicians see every day. A PT who regularly works with Boston runners is more likely to understand why symptoms flare during downhill volume, why winter treadmill mileage changes mechanics, or why a postpartum runner may need both pelvic floor support and a graded return to impact.
Joint Ventures Physical Therapy provides 1-on-1 physical therapy across Greater Boston, including Back Bay, Kenmore Square, Fort Point and Seaport, Downtown Boston, and nearby neighborhoods. Services include running performance evaluations, trigger point dry needling, pelvic floor therapy, vestibular and balance care, orthotic fitting, and wellness follow-up.
That range matters in difficult cases. A runner with recurring patellofemoral pain may need gait changes and strength work. A postpartum runner may need pressure management, pelvic floor treatment, and a slower impact build. A runner with repeated ankle injuries may also need balance testing and confidence rebuilding on uneven ground. The right clinic can sort out those differences and build the plan around them.
Choose the clinic that can match your goal, your schedule, and the actual complexity of your case. Fast promises are easy to market. A clear assessment and a plan that holds up over weeks of running is what gets people back on the road.
Take the First Step Back to Pain-Free Running
It is 6 a.m. in Boston, and you are standing at the curb deciding whether this run will help or set you back again.
That is the hardest part for many runners. Pain matters, but uncertainty is what stalls progress. You are left guessing whether rest is helping, whether your form is contributing, and whether the next workout is a smart test or one more setback before marathon training, a fall race, or a long-awaited PR.
A stronger rehab process removes that guesswork. It examines how you run, how much load you tolerate, how you recover between sessions, and what you are trying to get back to. It also accounts for the cases generic plans often miss, including postpartum return to impact, repeated flare-ups, and runners who did not improve with previous care. In Boston, that matters. The runner training through winter treadmill miles, Heartbreak Hill prep, or uneven sidewalks does not need generic advice. They need a plan built for the demands in front of them.
What a better outcome looks like
A good result is more than lower pain at rest.
It means:
- You understand what drove the injury
- You know which changes matter for your body
- You have a progression you trust
- You return to running with better capacity, not just fewer symptoms
That may include gait changes. It may include calf and hip loading, pelvic floor treatment for a postpartum runner, or tools like dry needling and blood flow restriction when they fit the problem. The point is not to throw every treatment at you. The point is to choose the right ones, measure the response, and keep building toward pain-free miles.
If you have been waiting for the pain to disappear on its own, it is time to get a clearer answer. A focused evaluation can show what is driving symptoms, what training you can keep, and what needs to change now so you can return to running with confidence.
If you’re ready to stop guessing, book an evaluation with Joint Ventures Physical Therapy. With 1-on-1 care and convenient Greater Boston locations, it is a practical next step for runners who want a clear plan back to pain-free miles.


