The phone call usually comes after a blur of sirens, scans, and unfamiliar words. A family member says, “They told us it’s a broken neck,” and everything after that sounds muffled. Patients feel it too. Even when they’re awake and talking, the diagnosis lands with a kind of shock that makes every next step feel huge.
That reaction makes sense. A cervical fracture is serious. But serious doesn’t mean hopeless, and it doesn’t mean recovery is random.
Broken neck recovery is usually a staged process. First comes protection and medical stabilization. Then healing. Then careful rebuilding. The people who do best usually aren’t the ones trying to rush through it. They’re the ones who understand what each phase is for and commit to it.
As physical therapists, we spend a lot of time helping patients and families translate the medical plan into real life. What does the brace mean for sleeping? How do you get dressed without twisting? When is stiffness normal, and when is it a warning sign? When can you drive, work, train, or carry your child again?
Those answers matter because recovery isn’t just about waiting for a bone to heal. It’s about protecting the injury while keeping the rest of the body, and the person, moving forward.
Your Guide Through Broken Neck Recovery
The first days after a cervical fracture are often the hardest emotionally. You may be hearing terms like “stable,” “unstable,” “fusion,” “halo,” or “neurological exam” while trying to process fear, pain, and lack of control.
Families often want the same thing right away. They want a map.
That map usually starts with one important truth. A broken neck recovery journey is active, even when it looks quiet from the outside. You may be in a collar. You may be waiting on imaging. You may have strict restrictions. But there’s still a plan, and every part of that plan has a purpose.
One patient described the early stage to me as “feeling like my whole life got put in a brace.” That’s accurate in one sense. Your world gets smaller for a while. But good rehab gradually expands it again.
What helps in the beginning
A few things consistently make the first stretch more manageable:
- Clear explanations: Patients do better when someone explains what the injury is, what’s protected, and what’s temporarily off-limits.
- One step at a time thinking: Focusing on this week works better than trying to predict every detail of the next year.
- Team-based care: The surgeon or trauma team handles the medical stability. PT and OT help turn that plan into safe daily function.
- Early education: Understanding movement precautions early prevents a lot of avoidable setbacks.
If you’re new to orthopedic rehab, it can help to understand what ortho physical therapy involves in plain language. It’s not just exercise. It’s guided problem-solving for healing tissue, pain, strength, mobility, and return to life.
You don’t need to solve the whole recovery at once. You need the right next decision, repeated consistently.
That’s how progress usually happens. Not in one dramatic leap. In protected, well-timed steps.

Understanding Your Cervical Fracture Injury
“Broken neck” sounds like one injury, but it isn’t. It’s a broad term for a fracture involving one of the seven vertebrae in the cervical spine.
A key question isn’t just whether the neck is broken. It’s how it’s broken, where it’s unstable, and whether the spinal cord or nerves are involved.
Stable versus unstable fractures
A simple way to think about it is to picture the neck like a structural support system.
A stable fracture is more like a crack in one part of the structure where the overall alignment still holds. The bone needs protection and time, but the spine remains sufficiently supported.
An unstable fracture is different. The alignment may be disrupted, the injured segments may move in ways they shouldn’t, and the risk to the spinal cord is higher. That’s when doctors start talking about rigid immobilization, a halo, or surgery.
How doctors decide on treatment
The emergency phase focuses on preventing extra movement and finding out exactly what happened. Imaging and neurological testing guide the plan.
That plan usually falls into one of two broad paths:
| Injury path | Typical medical approach | Why |
|—|—|
| Stable fracture | Brace or collar, close follow-up, gradual rehab later | Protect the bone while it heals without disrupting alignment |
| Unstable fracture | Halo, surgical fixation, or fusion | Restore stability and protect the spinal cord |
The reason early decision-making matters is clear in outcome data. In a 15-year study of over 10,000 patients with cervical spine fractures, the overall mortality rate during initial hospitalization was 9.87%. One-year mortality was 30% for non-intervened patients, 26% with halo placement, and 19% with surgical fixation, which shows why expert initial care matters (PMC study on cervical spine fracture outcomes).
That doesn’t mean every patient needs surgery. It means the right treatment choice, made early, matters.
Why the first diagnosis can feel confusing
Families often hear several related terms at once. Fracture. Dislocation. Cord compression. Neurological deficit. Each one changes the picture.
Some patients have a fracture with no cord damage. Others have a fracture plus nerve irritation or spinal cord injury. Those are very different recoveries.
For people trying to understand how trauma can affect the neck more broadly, this overview of whiplash and other neck injuries can help clarify how different neck injuries vary in severity and mechanism.
Clinical reality: The label “broken neck” doesn’t tell you the prognosis by itself. Stability, alignment, cord involvement, age, and baseline health shape the road ahead.
That’s why two people can have the same frightening diagnosis and very different treatment plans.
The Critical Immobilization and Healing Phase
Many people underestimate this stage. They assume nothing meaningful happens until the brace comes off.
In practice, this phase shapes the rest of recovery.
When a surgeon prescribes a rigid collar or halo, the goal is straightforward. Keep the injured area protected long enough for bone healing and surgical stabilization to take hold. If the fracture is unstable or has required fixation, too much motion too early can compromise healing.
What immobilization is doing for you
Immobilization is restrictive, but it serves a clear purpose. It reduces unwanted movement at the injured levels so the body can heal in a controlled position.
If surgery was required for an unstable fracture, fusion rates reach 95% to 98% at 6 months according to the cited recovery data, and post-op physical therapy can begin with gentle, therapist-guided isometrics as early as Week 2. That same source notes early intervention can cut the incidence of chronic pain by 50% (recovery time for a broken neck).
The important takeaway is that protection and rehabilitation are not opposites. They work together.
What PT does before your neck is moving much
Early rehab during broken neck recovery doesn’t look like neck strengthening class. It’s more targeted than that.
A therapist may focus on:
- Breathing mechanics: Pain, fear, and bracing often make people breathe shallowly and hold tension through the shoulders and jaw.
- Shoulder and arm mobility: Stiff shoulders can become a major secondary problem while the neck is immobilized.
- Walking and transfers: Getting in and out of bed, standing up, and using stairs safely matter right away.
- Positioning: Small changes in pillow setup, chair support, and arm support can reduce strain significantly.
- Circulation and deconditioning prevention: The longer someone moves less, the more whole-body weakness becomes part of the problem.
Occupational therapy often becomes invaluable here.
What OT changes in daily life
Patients are often surprised by how many basic tasks become awkward in a collar or halo.
OT helps with the practical mechanics of daily life:
- Dressing: Choosing clothing that doesn’t require overhead pulling or neck twisting
- Bathing and grooming: Organizing tools and positions so you can stay within precautions
- Eating: Managing posture and setup if swallowing or fatigue is an issue
- Household function: Reaching, carrying, cooking, and work-from-home setup
- Energy use: Doing less at once so symptoms don’t spike for the rest of the day
A lot of early success comes from accepting temporary adaptations instead of fighting them.
During immobilization, the goal isn’t to prove toughness. The goal is to heal cleanly while keeping the rest of your body as ready as possible for the next phase.
What tends to work and what doesn’t
Here’s the honest trade-off. Patients who respect restrictions often feel frustrated in the short term. Patients who test the limits too early often pay for it with more pain, slower progress, or medical setbacks.
A few patterns show up again and again:
| Usually helps | Usually backfires |
|---|---|
| Following brace rules exactly | “Just a quick stretch” outside precautions |
| Short, frequent walks | Long periods in bed unless medically necessary |
| Using adaptive tools | Forcing normal routines too soon |
| Addressing shoulder and mid-back stiffness early | Ignoring secondary pain until it becomes severe |
This phase can feel slow. It isn’t wasted time. It’s where stability, confidence, and safe habits start.
Your Phased Physical Therapy Rehabilitation Journey
Once your physician confirms enough healing, rehab becomes more active. This is the stretch where patients often feel hopeful and impatient at the same time.
That mix is normal. You’re moving more, but the neck still doesn’t feel like your neck yet.
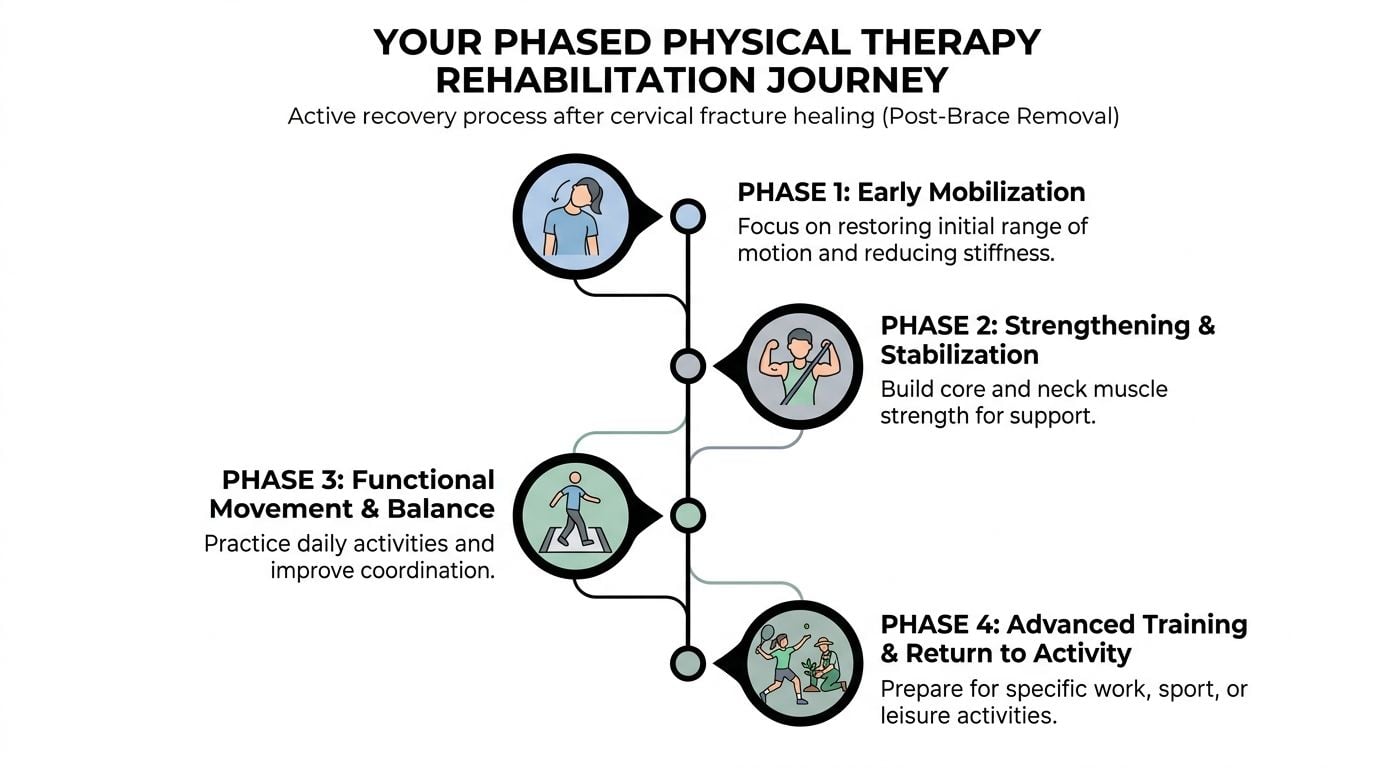
Phase one early mobilization
The first goal after clearance is simple. Restore movement without provoking the tissues that are still healing.
This phase usually includes gentle, specific range-of-motion work, not aggressive stretching. We’re looking for clean movement, not maximum movement. Patients often try to “push through” stiffness here. That usually creates guarding.
A better approach is to retrain motion gradually, with attention to breathing, jaw relaxation, shoulder position, and symptom response.
Common priorities include:
- Rotation for daily function: Looking left and right without substituting through the trunk
- Flexion and extension tolerance: Reintroducing small arcs of motion safely
- Scapular mechanics: If the shoulder girdle is moving poorly, the neck pays for it
- Pain education: Learning the difference between stiffness and a true aggravation
Phase two strengthening and stabilization
Once motion is improving, we shift toward support. The neck relies on a deep muscular system for control, and that system often gets inhibited after trauma, surgery, bracing, or pain.
Isometrics, postural retraining, and deep neck flexor work become central here. The work can look deceptively easy. It isn’t. Good control in a small range is often harder than people expect.
The progression matters. Patients usually do better when exercises are dosed precisely and advanced only when the quality is there.
A useful benchmark comes from cervical fracture rehab data. The intermediate phase, weeks 6 to 12, begins after imaging confirms fusion stability and progresses from isometric holds to active-assisted motion. The goals are 50% of pre-injury range of motion and a 30% reduction on the pain scale, and 85% to 95% of patients achieve full functional recovery in that context (cervical fracture rehab phases).
Phase three functional movement and balance
Many patients expect recovery to be about pain and range alone. Then they stand up, turn their head while walking, and realize they feel off.
That’s common. The neck helps the body understand position, balance, and motion in space. After injury, surgery, or prolonged guarding, those systems often need retraining.
This phase may include:
- Gait work: Walking while turning the head, changing speed, or navigating busy environments
- Sensorimotor drills: Rebuilding the neck’s position sense
- Vestibular integration: For patients dealing with dizziness, visual sensitivity, or motion intolerance
- Functional lifting: Learning to use the whole body instead of overworking the upper traps and neck
If dizziness or visual motion sensitivity is part of your picture, these neck exercises for vertigo can help explain how neck and balance symptoms sometimes overlap.
What I want patients to know: Feeling weak is expected. Moving poorly is common. Accepting sloppy mechanics because “at least I can do it” is what keeps problems around.
Phase four return to activity
Rehab becomes personal in this phase.
A desk worker needs one set of skills. A parent lifting a toddler needs another. A runner, swimmer, hockey player, CrossFit athlete, or musician needs even more specific preparation.
The neck has to tolerate real life again. That means building capacity for duration, impact, reaction time, and unpredictable movement.
A return-to-activity phase often includes:
| Goal | What rehab usually targets |
|---|---|
| Desk work | Sitting tolerance, screen height, arm support, turn-and-look tasks |
| Parenting | Safe lifting mechanics, floor transfers, carrying strategies |
| Gym return | Pulling, pressing, hinging, and breathing without neck dominance |
| Sport | Reaction drills, load tolerance, rotational control, confidence |
The most successful returns are gradual. Patients who jump from “I feel better” to full training usually expose weak links quickly.
Broken neck recovery gets better when rehab matches the life you’re trying to get back to, not just the injury you had.
Setting Realistic Timelines and Knowing the Red Flags
Patients ask about timelines early, and for good reason. You want to know when life will feel recognizable again.
The honest answer is that recovery moves on two clocks. One is tissue healing. The other is functional recovery. They overlap, but they’re not identical.
A bone or fusion can be progressing appropriately while the person still feels stiff, tired, or unsteady. That doesn’t mean something is wrong. It means healing and performance are different milestones.
Common Timeline Experiences
Several broad patterns are common.
Early healing often feels restrictive and tiring. Even simple tasks can take more planning than expected.
The next stretch usually brings more motion and less fear, but also reveals deficits that were hidden during immobilization. Weakness, dizziness, posture fatigue, and poor endurance often show up here.
Later recovery is where patients build consistency. That means tolerating longer days, handling work or school, and moving more normally without symptom spikes.
For neurological recovery, timing matters. The most significant neurological recovery from a broken neck injury typically happens within the first 6 to 9 months, with the most rapid gains in the first 3 months (prognosis of cervical fractures in older adults).
That matters because people often wait for symptoms to “settle” before engaging fully in rehab. In many cases, that’s the wrong instinct. When the medical team says it’s safe, targeted therapy during that window can make a meaningful difference.
Why comparisons can mislead you
Patients compare themselves to friends, online stories, and even other fracture recoveries. That usually creates more anxiety than clarity.
For example, bone healing questions come up across many injuries, and general resources on healing timelines for stress fractures can be useful for understanding why bone recovery tends to require patience. But a cervical fracture has its own mechanical demands, safety concerns, and neurological considerations. It isn’t something you can benchmark against an ankle or foot injury.
Red flags that need quick attention
Some symptoms are expected. Others deserve immediate communication with your surgeon, physician, or therapist.
Call promptly if you notice:
- New numbness or tingling: Especially if it’s spreading or accompanied by weakness
- Worsening arm or leg weakness: Not just fatigue, but a noticeable drop in strength
- Severe increase in neck pain: Especially after a movement, stumble, or fall
- Loss of coordination or balance: If it’s suddenly worse than your recent baseline
- Changes in bowel or bladder function: These require urgent medical attention
- Severe headache, fever, or unusual swelling: Particularly after surgery
What’s often normal, even if it’s frustrating
A few things commonly worry patients but often fit the expected course:
| Common but often expected | Worth monitoring closely |
|---|---|
| Morning stiffness | New neurological symptoms |
| Fatigue after therapy | Sudden sharp symptom escalation |
| Fear with first bigger movements | Repeated loss of balance |
| Soreness in shoulders and upper back | Progressive weakness |
Recovery should challenge you. It should not surprise you in dangerous ways.
That’s the standard I use clinically. Progress can feel hard. It shouldn’t feel mysterious.
Returning to Your Life Work Sport and Everything In Between
Getting told the fracture is healed is a relief. It’s not the same thing as being ready for normal life.
Many individuals discover that the true milestone isn’t “the scan looks good.” It’s “I trust my body again.”
Returning to work
Desk work seems easy until you try it with a recovering neck. Long screen time, poor monitor height, unsupported arms, and shallow breathing can create a surprising amount of strain.
What tends to help:
- Monitor at eye level: So you’re not living in sustained flexion
- Arm support: Forearms supported on the desk or chair arms reduce neck loading
- Frequent resets: Short posture changes beat heroic attempts to sit perfectly all day
- Task batching: Alternate computer work, calls, and standing tasks when possible
For jobs that involve lifting, driving, patient care, construction, or field work, return is more complex. Those roles require neck motion, reaction time, strength, and endurance under real-world demands. Rehab should reflect that before full return.
Returning to the gym
The gym is where motivated patients often make their biggest mistake. They feel better, so they go back to old weights and old habits.
A smarter return starts with movement quality. Can you row without shrugging? Can you hinge without craning your head? Can you press without turning your neck into the prime mover?
A few principles matter:
- Rebuild patterns first: Pull, push, squat, carry, hinge
- Use pain as information: Don’t chase soreness, and don’t panic at every sensation
- Respect fatigue: Form usually breaks before motivation does
- Progress load slowly: The neck often tolerates less than your legs and lungs are ready for
Returning to sport
Sport return depends on more than strength. Athletes need rotational control, visual tracking, reaction under speed, and confidence in contact or unpredictable environments.
That’s why sport-specific rehab matters. A runner may need head-turn tolerance, stride rhythm, and arm swing symmetry. A tennis player needs rotational loading. A hockey player or soccer player needs quicker head movement and much higher environmental demand.
This is a helpful demonstration of movement-focused rehab principles for active patients:
If your goal is a full return to training or competition, sports-specific planning matters more than generic exercise. This overview of sports medicine and rehab is a good starting point for understanding how clinicians bridge that gap.
The overlooked part of recovery
Family roles matter too.
Parents need strategies for carrying children without constant upper-trap tension. Commuters need plans for backpacks, stairs, and public transit. Hikers need graded exposure to uneven ground and longer duration. Musicians need endurance in postures that don’t look athletic but absolutely are.
The finish line in broken neck recovery isn’t just less pain. It’s being able to do your own life with confidence and control.
That standard is higher, and it’s the one worth aiming for.
Common Questions From Our Boston Patients
Can I do PT somewhere different from where I had surgery
Yes, in most cases. That’s common.
Your surgeon handles imaging, precautions, and medical follow-up. Your physical therapist handles the day-to-day progression of mobility, strength, balance, and functional return. What matters most is that the PT clinic gets clear operative notes, restrictions, and updates when your status changes.
Patients often worry that care gets fragmented across systems. It doesn’t have to. Good clinics communicate well and adjust the plan around the surgeon’s instructions.
Will insurance cover enough therapy
Sometimes yes, sometimes not enough for the full arc of recovery.
That’s one reason one-on-one visits matter. When visit counts are limited, each session needs to be focused, specific, and tied to meaningful goals. Patients generally do better when the clinic also helps with authorizations, progress notes, and timing of re-evaluations rather than leaving them to figure it out alone.
If your benefits are tight, ask direct questions early. How many visits are available. Is prior authorization needed. What happens after the initial approval. Those practical details affect momentum.
I live in the city and walk everywhere. Does that change anything
It does.
City patients often rely on walking, stairs, backpacks, train platforms, and quick head turns in crowded environments. Those demands can expose symptoms earlier than suburban driving-based routines.
That isn’t a problem. It just means rehab should train for it. We often have patients practice turning, scanning, carrying, and navigating busier visual environments before they feel fully ready. That preparation helps.
When can I run again
That depends on fracture stability, healing status, symptoms, and how much impact your neck is tolerating.
Running is not just a cardiovascular activity. It’s repeated impact plus arm swing plus trunk rotation plus visual scanning. Some patients can build back to it gradually. Others need more time before impact feels clean.
The right question isn’t “Can I jog yet?” It’s “Can I walk briskly, turn my head, manage posture fatigue, and handle light loading without a symptom spike?” If those pieces aren’t there, running usually isn’t ready either.
Can I care for my kids during recovery
Usually yes, but often not the way you’re used to at first.
The biggest issues are lifting, floor transfers, awkward reaches, and fatigue. Parents often do best with a temporary plan. More seated play. Fewer rushed pickups. Better body positioning for car seats, baths, and bedtime routines.
That can be emotionally hard. It’s still smarter than trying to power through and paying for it later.
How do I know if my clinic is the right fit
Look for a clinic that gives you uninterrupted time, clear reasoning, and a plan that changes as you improve.
You should leave visits understanding what you’re working on, why it matters, and what to watch for before the next session. If treatment feels generic, rushed, or disconnected from your goals, that’s a problem. Broken neck recovery is too important for autopilot care.
If you need help navigating broken neck recovery, Joint Ventures Physical Therapy offers personalized 1-on-1 care across Greater Boston, with expert PT and OT support for orthopedic rehab, balance issues, sports return, and the everyday demands that come after a serious cervical injury.



